Sunday, May 30, 2010
Rope Climbing, how to climb a rope efficiently (if you can find a rope...)
Follow @mcphoo
Tweet
Ever climbed a rope? I haven't yet. But it *seems* like such the complete athletic movement - like a pull up that keeps on going, no? So this is a post to help folks prep for your own rope climbing ascent.
 Partial History. It turns out that once upon a time - from between the 1860's to 1932 rope climbing was an olympic event. It persisted as a college competition sport into the 1960's.
Partial History. It turns out that once upon a time - from between the 1860's to 1932 rope climbing was an olympic event. It persisted as a college competition sport into the 1960's.
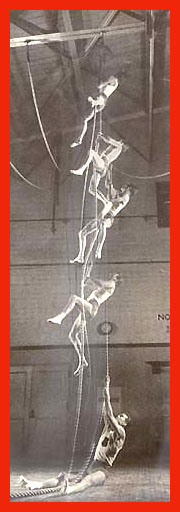
John Gill put together a wonderful overview of both the history and the specs of the competition. Please visit these pages - the content and images are lovely, and its fabulous to read the descriptions from various periods of the respect and pleasure experienced by authors who obviously enjoyed practicing this movement. Citing from there, Gill quotes a wonderful text on gymnastics from the 50's that describes climbing this way:
Modern Practice. Apparently in 1993, it started a resurgence in the Czech republic that is still going strong, as demonstrated in this 2007 vid below:
 Kids Resurgence. Perhaps more excitingly, rope climbing is apparently also making a come back in kids gymnastics classes as part of the National Elite Physical Abilites testing (pdf), at least in the states. And the cool thing is, form here - of keeping the legs in pike position - is part of the practice - so no leg help; all upper body and core.
Kids Resurgence. Perhaps more excitingly, rope climbing is apparently also making a come back in kids gymnastics classes as part of the National Elite Physical Abilites testing (pdf), at least in the states. And the cool thing is, form here - of keeping the legs in pike position - is part of the practice - so no leg help; all upper body and core.
Very cool to see girls do this so well - don't stop!
Getting Practical. Here's some awesome rope climbing teaching tips for starting with kids (how well do these translate to adults?)
Adult Tips One place where rope climbing is used more as a physical readiness test than as a competition is in the French Foreign Legion, where climbing a rope multiple times with 24kg of gear is not unknown. So here's a french foreign legion rope climbing tip.
I can confirm that this approach has been tested out by experience rope climbers who found that it made a climb "ridiculously easy"with the added tip to "stay close to the rope" and "look down a bit"
I'm keen to try rope climbing. i imagine sitting down legs out, and rather staying down. Actually, part of the challenge for me is just finding a place with a rope. Our uni gym doesn't have one (does yours?). I've run trails where there are pull up bar stations at points on the trail, but not rope climbing ones - perhaps it's a health and safety fear? Work was not happy about a rope slung down between an open area between two floors. Perhaps if it had had decorative ivy?
Climbing Simulation: Update 2011 - crosscore War Machine -
Ok since i wrote this post, i've found a way to practice rope climbing without a rope. It's called (ahem) the "war machine" made in the US by some awesome guys. Really. Awesome. If you scroll in to 55secs, the vid below shows the climbing simulation (but the whole vid is so good, you just might want to watch the whole thing.
The cool thing is that with the WM we're able to practice the techniques for climbing recommended above. Wicked. Starting with feet on a box or ball or jammed into the wall is also great. If you're interested in the WM in the US avail right from cross core; in the UK avail from Balance Performance. In either case, tell 'em dr mc sent you and they'll be happy happy.
General Queries: Do you climb a rope? if so, do you keep your legs piked out? where do you practice? would you agree it's technique?
Look forward to hearing from you.
Related Posts - in strength as practice
Partial History. It turns out that once upon a time - from between the 1860's to 1932 rope climbing was an olympic event. It persisted as a college competition sport into the 1960's.John Gill put together a wonderful overview of both the history and the specs of the competition. Please visit these pages - the content and images are lovely, and its fabulous to read the descriptions from various periods of the respect and pleasure experienced by authors who obviously enjoyed practicing this movement. Citing from there, Gill quotes a wonderful text on gymnastics from the 50's that describes climbing this way:
Competitive rope climbing is truly an art and a skill by itself. It does not involve all the intricacies or maneuvers of apparatus work yet the art of climbing can be detailed and exacting in nature. A great deal of practice is involved to produce a champion rope climber. Since the record for climbing a rope 20' high with the hands alone is under 3 seconds it is easily understood why considerable practice is necessary for top performances. (sited as from Newt Loken & Robert Willoughby in the Complete Book of Gymnastics, 1959.)That's a pretty compelling description of a skill-based rather than just strength based practice.
Modern Practice. Apparently in 1993, it started a resurgence in the Czech republic that is still going strong, as demonstrated in this 2007 vid below:
Kids Resurgence. Perhaps more excitingly, rope climbing is apparently also making a come back in kids gymnastics classes as part of the National Elite Physical Abilites testing (pdf), at least in the states. And the cool thing is, form here - of keeping the legs in pike position - is part of the practice - so no leg help; all upper body and core.Very cool to see girls do this so well - don't stop!
Getting Practical. Here's some awesome rope climbing teaching tips for starting with kids (how well do these translate to adults?)
Adult Tips One place where rope climbing is used more as a physical readiness test than as a competition is in the French Foreign Legion, where climbing a rope multiple times with 24kg of gear is not unknown. So here's a french foreign legion rope climbing tip.
I will now reveal the secret to the dreaded rope climb. RaiderDingo was the closest to the technique. It is very simple, and has little to do with upper-body strength. It is 90% technique. I did miss several meals (we had to climb it every day before midday meal) before I studied the guys who scooted right up the damn thing. When I saw how they did it, I almost laughed at myself. I truly believe that EVs should have to figure it out for themselves, like we anciens did. But, with all of the "upper-body strength" answers, I feel that I must give this out to the wannabes--I seldom reveal Legion secrets, as my brother anciens should know by now, so take this as Primo Info from one who knows.

Everyone makes the same mistake--they reach up as high as they can, and start to pull themselves up--this is wrong and will wear you out before you get 1 meter. The correct way is to start with both hands directly in front of your nose--elbows at 45% at all times--take short steps with your hands, keeping them directly in front of your nose at all times--NEVER, I repeat NEVER straighten your arms. Some of the testing requires that you climb it twice, without ever touching the ground between the two climbs, we had to go up once, come back down, and without setting either foot on the ground, go right back up. If you use this technique, you will have no trouble going up and down several times. I am 6 feet and 1 inch tall, slim, with ZERO upper-body strength--I could barely do 3 pull-ups, but once I got the TECHNIQUE, I never had any problem with the rope. In fact, during the testing, I started up the rope for the 3rd time without touching ground, and the Sgt. had to stop me. I think he was afraid that I was giving the secret away.
It is my OPINION, that they are not testing upper-body strength, as much as MENTAL CAPACITY. So, les gars, there you have it. If you doubt the simplicity of this, just try it at your local gym--believe me, you will be amazed. This is the only secret I will ever give away, so take it to heart and savor your victory when you astonish the cadre by scooting right up the damned dreaded rope the very first time. I do expect expensive cadeaux from all EVs who trust me and use the technique. I hope this will be the end of the "rope" questions. Tex __________________
Les hommes comme vous, je ne refuser rien.
I can confirm that this approach has been tested out by experience rope climbers who found that it made a climb "ridiculously easy"with the added tip to "stay close to the rope" and "look down a bit"
I'm keen to try rope climbing. i imagine sitting down legs out, and rather staying down. Actually, part of the challenge for me is just finding a place with a rope. Our uni gym doesn't have one (does yours?). I've run trails where there are pull up bar stations at points on the trail, but not rope climbing ones - perhaps it's a health and safety fear? Work was not happy about a rope slung down between an open area between two floors. Perhaps if it had had decorative ivy?
Climbing Simulation: Update 2011 - crosscore War Machine -
Ok since i wrote this post, i've found a way to practice rope climbing without a rope. It's called (ahem) the "war machine" made in the US by some awesome guys. Really. Awesome. If you scroll in to 55secs, the vid below shows the climbing simulation (but the whole vid is so good, you just might want to watch the whole thing.
The cool thing is that with the WM we're able to practice the techniques for climbing recommended above. Wicked. Starting with feet on a box or ball or jammed into the wall is also great. If you're interested in the WM in the US avail right from cross core; in the UK avail from Balance Performance. In either case, tell 'em dr mc sent you and they'll be happy happy.
General Queries: Do you climb a rope? if so, do you keep your legs piked out? where do you practice? would you agree it's technique?
Look forward to hearing from you.
Related Posts - in strength as practice
- asha wagner - pistoling, pull up'ing and pressing a 24kg kb
- michael castriovanni interview - tossing kettlebells with a partner
- hanging leg raise: technique first then strength?
- Pull ups 101 - how to, in many ways
- War Machine in Training - with Rannoch Donald
Saturday, May 29, 2010
How to Get outsdide and Move better fast: right water, safe barefeet and sun cover, rather than sun screen
Follow @mcphoo
Tweet
Now that we've seen and felt the sun in the UK/EU for a few days, one turns there thoughts to summer. And summer means sweat, and sweat means hydration, so a few notes about hydration, sun screen and barefooting.
Why these three?
we'd like to stay out side for fresh air - and not burn like a crispy critter OR be outside and NOT get the vitamin D we need; we'd likely like to move better and hydration actually helps our bodies move better. really. and while our muscles, skin and fascia move better with some H2O, we move better when we let our joints (in parts like our feet) move as designed. Sounds right, right?
So a few thoughts/tips on water, feet and sun (screen).

a quick note about hydration: amount
here's a few pointers about how much water to drink - it may be less than we usually think:
Water is a biggie for lots of reasons, but one is that it lets muscles and fascia (our connective tissue) actually move better. A hydrated body is a happy body.
Too much of a good thing? And if you've been chugging gallons for awhile, any extreme can be a problem - with too much water consumption (rare) it's called hyponatremia:
About Sun Screen
Well what can i say? time to think different, as it were.
Likewise those spray on tans (and tanning beds) aren't necessarily helping. Seems we need to relearn our relationship to the sun, sanely.
About running about barefoot or near barefoot. Nothing like splish splashing barefoot; or feeling the grass (or mud) between one's toes. And it's great to do with minimal shodness - yes i'm thinking vibram fivefingers (and i keep hearing great things about the bikilia's too - will report when i get a chance to try them, too). Here's a few starters.

 In rare rare cases, pain (like in a toe or heal) may be something else showing up that's been in train for awhile. There's stuff called freiburgs syndrome and heal spurs. Pain is a signal to change something; sometimes we need help to figure out how to make that change. If you have sharp pain in your foot at any point, see your doc.
In rare rare cases, pain (like in a toe or heal) may be something else showing up that's been in train for awhile. There's stuff called freiburgs syndrome and heal spurs. Pain is a signal to change something; sometimes we need help to figure out how to make that change. If you have sharp pain in your foot at any point, see your doc.
Cramps? Shin SplinAnd if you are all gung ho in your new not suede shoes, and find yourself getting cramps, here's a few notes on what may be happening, and suggestions on how to deal with that. Remember: stretching is for dealing with the cramp; dun't work in avoiding 'em.
But on the up side
Reasonable hydration, reasonable sun exposure/sun cover, and reasonable movement towards moving as we're designed to move, greater happiness is ours. really. Water helps us move better; better foot mobility helps us move better. Moving helps us feel better.
Amen!
Related Notes:
Why these three?
we'd like to stay out side for fresh air - and not burn like a crispy critter OR be outside and NOT get the vitamin D we need; we'd likely like to move better and hydration actually helps our bodies move better. really. and while our muscles, skin and fascia move better with some H2O, we move better when we let our joints (in parts like our feet) move as designed. Sounds right, right?
So a few thoughts/tips on water, feet and sun (screen).

a quick note about hydration: amount
here's a few pointers about how much water to drink - it may be less than we usually think:
water by metabolic rate: for every 100kcal of metabolic rate, 80-110mL wateror
So 2000kcal mr = 1.6-2L a day.
every KG bw = 30-40mL of water, so 50kg= 1.5-2L a day; 100kg 3-4L
Generally, consensus seems to be around 3L (12cups) a day, with 1L coming from food, so 2L (8cups) from drinking water.Also exercise usually (duh) ups the requirements. Here's what the ACSM recommends for exercise, sun and hydration: chug it, rather than sip it; don't rely on thirst, but the goal is still simply "replacing body fluid loss during exercise is to maintain normal hydration" - not overdoing it. There's some good recs about carb/electrolyte intake during exercise to offset fatigue, too.
This is modified by body size (not thirst - thirst is similar to when the oil gage is on RED).
Water is a biggie for lots of reasons, but one is that it lets muscles and fascia (our connective tissue) actually move better. A hydrated body is a happy body.
Too much of a good thing? And if you've been chugging gallons for awhile, any extreme can be a problem - with too much water consumption (rare) it's called hyponatremia:
Common symptoms of hyponatremia include fatigue, irritability, headache, and water retention, loss of appetite, and nausea or vomiting.Just had a discussion recently with a person who said that their fatigue was found to be down to excessive water intake. Went to a more reasonable (2L for them) a day level and voila. Feeling betterness ensues. But again, this condition is pretty rare.
About Sun Screen
Well what can i say? time to think different, as it were.
- sunscreen will kill you (i know i was surprised)
Likewise those spray on tans (and tanning beds) aren't necessarily helping. Seems we need to relearn our relationship to the sun, sanely.
About running about barefoot or near barefoot. Nothing like splish splashing barefoot; or feeling the grass (or mud) between one's toes. And it's great to do with minimal shodness - yes i'm thinking vibram fivefingers (and i keep hearing great things about the bikilia's too - will report when i get a chance to try them, too). Here's a few starters.
- fitting vffs and injinji toe socks
- relation to pose/chi running
- cheap massage (especially in semi muddy pebbly trails)
 In rare rare cases, pain (like in a toe or heal) may be something else showing up that's been in train for awhile. There's stuff called freiburgs syndrome and heal spurs. Pain is a signal to change something; sometimes we need help to figure out how to make that change. If you have sharp pain in your foot at any point, see your doc.
In rare rare cases, pain (like in a toe or heal) may be something else showing up that's been in train for awhile. There's stuff called freiburgs syndrome and heal spurs. Pain is a signal to change something; sometimes we need help to figure out how to make that change. If you have sharp pain in your foot at any point, see your doc. Cramps? Shin SplinAnd if you are all gung ho in your new not suede shoes, and find yourself getting cramps, here's a few notes on what may be happening, and suggestions on how to deal with that. Remember: stretching is for dealing with the cramp; dun't work in avoiding 'em.
But on the up side
Reasonable hydration, reasonable sun exposure/sun cover, and reasonable movement towards moving as we're designed to move, greater happiness is ours. really. Water helps us move better; better foot mobility helps us move better. Moving helps us feel better.
Amen!
Related Notes:
- drink responsibly: get a refillable water bottle
- choosing a water bottle
- the b2d vibram fivefinger article index
- what is z-health?
Sunday, May 23, 2010
Weight Loss Ups your Power - if you're a competitive cyclist and not going nuts with the CR.
Follow @mcphoo
Tweet
 There's been a debate for some time as to whether or not "fasted cardio" is ok. There's a "fasted cardio roundtable" at t-nation discussing this, and good arguments on either side. The title of a recent article made me think "great - a specific study on fasted cardio with elite athletes" Here's the title: "Effects of caloric restriction and overnight fasting on cycling endurance performance." But alas, it's not about fasted cardio: it's about doing an exertion test after ONE night of fasted cardio after having been on a calorie restricted diet.
There's been a debate for some time as to whether or not "fasted cardio" is ok. There's a "fasted cardio roundtable" at t-nation discussing this, and good arguments on either side. The title of a recent article made me think "great - a specific study on fasted cardio with elite athletes" Here's the title: "Effects of caloric restriction and overnight fasting on cycling endurance performance." But alas, it's not about fasted cardio: it's about doing an exertion test after ONE night of fasted cardio after having been on a calorie restricted diet.
Not the most usual circumstance. Indeed, the study is interesting nonetheless for a couple of other related reasons: it's looking at the effects on performance of a protocol often used by cyclists before competetive race season when they need to drop some weight to improve their Power to Weight Ratio (PWR) - lighter on the bike but still driving the same power means get there faster, if not fasted.

So not exactly fasted cardio - as in regularly doing cardio in a fasted state. But there are *some* findings that may reasonably be extended - maybe - around fasted cardio. In particular the effects shown around perceived exertion in this condition and intriguingly fat utilization.
Here's the abstract
Here's the actual protocol during the study:
In the lab: the athletes did a submaximal two hour endurance ride (with ipods and music of their choice if they wished) on lab bikes set up just like their racing bikes with the following condition:
Results:
over the 25 days of their CR, they lost weight - in particular their body fat dropped but their lean mass was maintained. They had a 1.7 plus or minus. 5kg body weight loss, with a drop in bf% of 2.1 (plus or minus .4) %. Lean mass increased by 2.1%. No muscle mass loss. That's a plus of exercise while doing calorie reduction: lean mass hangs in.
in the lab: the fasted, post CR test showed no statisitcal difference in power output, Vo2max, resting metabolic rate (RMR), revolutions per minute. In otherwords, nothing performance wise changed - in particular, nothing changed netgatively - as a result of the CR and fasted state of the test.
One place there was a difference: PWR at 90 and 100% vo2max was significantly different post CR (it went up), though no PLWR (power to lean weight ratio) changes.
The authors suggest:
Two notable changes/surprises: first, that perceived exertion was LOWER after the CR period. And second, that despite doing a heavy work load after an 11 hour fast, fat oxidation (using fat as the main fuel for the workout) did not change from baseline. Now me, i must be missing something because both base line test and re-test post CR were the same: post 11 hour fast. But here's what the authors say about the fat oxidation non-change:
Practical Applications
The authors have some cautiously positive effects to report
In other words, there's some good results in terms of body comp and PWR from a pretty intense caloric restriction for three weeks, but we don't know what would happen if this was strung out or for that matter repeated at intervals anywhere into competetive season. This ain't a license to go nuts.
And it's also not much help when thinking about fasted cardio as a regular practice.What i'm not sure this study says is what the authors state in the abstract: that "Caloric restriction (up to 40% for 3 weeks) and exercising after fasting overnight can improve a cyclist's PWR without compromising endurance cycling performance" Caloric restriction for three weeks with regular workouts, sure, but one session of fasted endurance work? Maybe i'm reading this wrong, but that seems a bit of a stretch. All it seems one can say is that after three weeks of caloric restriction, a sub max endurance workout in a fasted state when done by elite athletes doesn't have any negative effects - on them.
On the plus side: one can work to weigh less and maintain power, thereby increasing power. And for sports, like life, where better body comp has a host of benefits, a three week nutritionally balanced calorie cut with maintained workouts - at least for seasoned athletes - can be effective. Does this approach transfer to non-competetive athletes? May be worth investigating.
Citations
Related Articles
Not the most usual circumstance. Indeed, the study is interesting nonetheless for a couple of other related reasons: it's looking at the effects on performance of a protocol often used by cyclists before competetive race season when they need to drop some weight to improve their Power to Weight Ratio (PWR) - lighter on the bike but still driving the same power means get there faster, if not fasted.

So not exactly fasted cardio - as in regularly doing cardio in a fasted state. But there are *some* findings that may reasonably be extended - maybe - around fasted cardio. In particular the effects shown around perceived exertion in this condition and intriguingly fat utilization.
Here's the abstract
Doesn't the above sound to you like the cyclists were doing both caloric restriction for three weeks AND doing fasted cardio at the same time? Well it turns out the only time we know that they did fasted cardio was on two test occaisions: before the diet started and at the end of the three week period
J Strength Cond Res. 2009 Mar;23(2):560-70.
Effects of caloric restriction and overnight fasting on cycling endurance performance.
Ferguson LM, Rossi KA, Ward E, Jadwin E, Miller TA, Miller WC.
Department of Exercise Science, The George Washington University, Washington, DC, USA. Abstract:
In addition to aerobic endurance and anaerobic capacity, high power-to-weight ratio (PWR) is important for cycling performance. Cyclists often try to lose weight before race season to improve body composition and optimize PWR. Research has demonstrated body fat-reducing benefits of exercise after fasting overnight. We hypothesized that fasted-state exercise in calorie-restricted trained cyclists would not result in performance decrements and that their PWR would improve significantly. We also hypothesized that substrate use during fasted-state submaximal endurance cycling would shift to greater reliance on fat. Ten trained, competitive cyclists completed a protocol consisting of baseline testing, 3 weeks of caloric restriction (CR), and post-CR testing. The testing sessions measured pre- and post-CR values for resting metabolic rate (RMR), body composition, VO2, PWR and power-to-lean weight ratio (PLWR), and power output, as well as 2-hour submaximal cycling performance, rating of perceived exertion (RPE), and respiratory exchange ratio (RER). There were no significant differences between baseline and post-CR for submaximal trial RER, power output, VO2, RMR, VO2max, or workload at VO2max. However, RPE was significantly lower, and PWR was significantly higher post-CR, whereas RER did not change. The cyclists' PWR and body composition improved significantly, and their overall weight, fat weight, and body fat percentage decreased. Lean mass was maintained. The cyclists' RPE decreased significantly during 2 hours of submaximal cycling post-CR, and there was no decrement in submaximal or maximal cycling performance after 3 weeks of CR combined with overnight fasting. Caloric restriction (up to 40% for 3 weeks) and exercising after fasting overnight can improve a cyclist's PWR without compromising endurance cycling performance.
Here's the actual protocol during the study:
For the CR period, subjects followed a fixed-macronutrient, calorie-restricted diet [this was set carbs, fats, proteins equivalent to a 40% reduction in total calories -mc] while maintaining their normal exercise training routines. None of the athletes were actively involved in strength training. Individual training plans typically involved base miles and some interval work, as it was still the off-season. Training was not standardized among athletes, because each athlete was a seasoned cyclist, accustomed to his or her own training regimen, and making changes to those plans could have produced chronic fatigue, muscle soreness, or altered the training volume to which each cyclist was accustomed-any of which could have led to unfavorable temporary adaptations that would have confounded their performance in their paired time trials.In other words, they were doing big calorie restriction and that's the only change to their training. We don't know if training actually changed in any way during this period - though participants were asked to keep things the same during the study as before in terms of these workouts. Ok, let's say that's all fine, then.
In the lab: the athletes did a submaximal two hour endurance ride (with ipods and music of their choice if they wished) on lab bikes set up just like their racing bikes with the following condition:
A metronome was used to ensure that subjects cycled at a constant 50 rpm to allow for consistent evaluation of workload. Subjects warmed up for 5 minutes at 100 W for men and 75Wfor women. The workload was incrementally increased by 50 Wevery 2.5 minutes. When HR reached 35 bpm below age-predicted maximal HR (220 bpm 2 age), or when the respiratory quotient exceeded 1, the workload was only increased by 25 Wevery 2.5 minutes until exhaustion. The subject cycled to exhaustion, ending the test voluntarily when he or she could no longer pedal or keep the 50-rpm cadence. Each subject wore a mouthpiece and nose clip, and ventilatory air was continuously analyzed forO2 consumption and CO2 production using the ParvoMedics system. Also, HR, RPE, and power output were recorded at the end of each stage throughout the test.
Results:
over the 25 days of their CR, they lost weight - in particular their body fat dropped but their lean mass was maintained. They had a 1.7 plus or minus. 5kg body weight loss, with a drop in bf% of 2.1 (plus or minus .4) %. Lean mass increased by 2.1%. No muscle mass loss. That's a plus of exercise while doing calorie reduction: lean mass hangs in.
in the lab: the fasted, post CR test showed no statisitcal difference in power output, Vo2max, resting metabolic rate (RMR), revolutions per minute. In otherwords, nothing performance wise changed - in particular, nothing changed netgatively - as a result of the CR and fasted state of the test.
One place there was a difference: PWR at 90 and 100% vo2max was significantly different post CR (it went up), though no PLWR (power to lean weight ratio) changes.
The authors suggest:
The increase in PWR was influenced by the significant decreases in body weight and percent body fat. Because there was no significant loss of lean body mass, the PLWRwas maintained. Thus, power was maintained not simply because of weight loss but because of the maintenance of fat-free mass. This increase in power output at high intensity levels, accompanied by a decrease in body weight, will provide the cyclist with more energy and power for improved uphill cycling performance.Overall then, the cyclists did get what they wanted: an improved Power to Weight Ratio: their power stays the same, but at a lighter weight. That translates potentially into getting the bike moving down the road faster.
Two notable changes/surprises: first, that perceived exertion was LOWER after the CR period. And second, that despite doing a heavy work load after an 11 hour fast, fat oxidation (using fat as the main fuel for the workout) did not change from baseline. Now me, i must be missing something because both base line test and re-test post CR were the same: post 11 hour fast. But here's what the authors say about the fat oxidation non-change:
Although we hypothesized that we would find a greater reliance on fat oxidation post-CR, particularly because RER [respiratory exchange rate - seeing which fuel is used more, carbs or fat -mc] - measuring has been previously shown to be lower in the fasted state (Aragón-Vargas LF 93, Knapik JJ88 ), this was not statistically supported. ...A possible explanation for the lack of a significant shift to fat metabolism is that the subjects were all highly trained endurance cyclists already and, as such, were able to use fat as a fuel more efficiently than if they had been untrained subjects.Hmm. Makes ya wonder.
Practical Applications
The authors have some cautiously positive effects to report
[The study results] suggests that CR (up to 40% for 3 weeks) and exercising after fasting overnight can improve a cyclist’s PWR without compromising endurance cycling performance. Furthermore, this study demonstrates that a shortterm period of moderately severe CR is not detrimental to the conditioning process. Athletes can continue to prepare for the upcoming race season in terms of endurance training while dieting to reduce body weight without losing significant muscle mass in the process. However, it is not known what would happen to performance if an athlete were to prolong his or her exposure to the CR beyond 3 weeks, or to repeat the 3-week exposure to CR with short intervals of balanced energy intake in between. The current data suggest that a protocol such as the one outlined in this report would be most appropriate if used in the off-season to increase PWR or during the season before a competition.
In other words, there's some good results in terms of body comp and PWR from a pretty intense caloric restriction for three weeks, but we don't know what would happen if this was strung out or for that matter repeated at intervals anywhere into competetive season. This ain't a license to go nuts.
And it's also not much help when thinking about fasted cardio as a regular practice.What i'm not sure this study says is what the authors state in the abstract: that "Caloric restriction (up to 40% for 3 weeks) and exercising after fasting overnight can improve a cyclist's PWR without compromising endurance cycling performance" Caloric restriction for three weeks with regular workouts, sure, but one session of fasted endurance work? Maybe i'm reading this wrong, but that seems a bit of a stretch. All it seems one can say is that after three weeks of caloric restriction, a sub max endurance workout in a fasted state when done by elite athletes doesn't have any negative effects - on them.
On the plus side: one can work to weigh less and maintain power, thereby increasing power. And for sports, like life, where better body comp has a host of benefits, a three week nutritionally balanced calorie cut with maintained workouts - at least for seasoned athletes - can be effective. Does this approach transfer to non-competetive athletes? May be worth investigating.
Citations
Ferguson LM, Rossi KA, Ward E, Jadwin E, Miller TA, & Miller WC (2009). Effects of caloric restriction and overnight fasting on cycling endurance performance. Journal of strength and conditioning research / National Strength & Conditioning Association, 23 (2), 560-70 PMID: 19197210
Aragón-Vargas LF (1993). Effects of fasting on endurance exercise. Sports medicine (Auckland, N.Z.), 16 (4), 255-65 PMID: 8248683
Knapik JJ, Meredith CN, Jones BH, Suek L, Young VR, & Evans WJ (1988). Influence of fasting on carbohydrate and fat metabolism during rest and exercise in men. Journal of applied physiology (Bethesda, Md. : 1985), 64 (5), 1923-9 PMID: 3292504
Related Articles
- 6mins to weight loss and fitness?
- Cardio levels when ya can't do HIIT
- HIIT intervals (on bikes) for fat loss
- Hill workouts - with kettlebells
- Respect the Fat
Building & Protecting Bone: Odd Angle Exercise, Resistance, Movement (and shaking) Work
Follow @mcphoo
Tweet
 A fear for many women is that as we age, we seem to be more vulnerable to the "Help Help, i've fallen and i can't get up" hip fracture and related. Awhile ago, i wrote about bone building, and what's known about strategies to keep it together and enhance it. Quick review: bone builds in response to demand. Woolf's law is "use it or lose it" - our bone is "remodeling" all the time. So while calcium, magnesium, zinc and vitamin d are all important, these nutrients alone don't really go into bone building mode unless there's demand on the bones. That means load. Likewise, even with strong bones, we don't stay upright if our movement is compromised by various aches and pains.
A fear for many women is that as we age, we seem to be more vulnerable to the "Help Help, i've fallen and i can't get up" hip fracture and related. Awhile ago, i wrote about bone building, and what's known about strategies to keep it together and enhance it. Quick review: bone builds in response to demand. Woolf's law is "use it or lose it" - our bone is "remodeling" all the time. So while calcium, magnesium, zinc and vitamin d are all important, these nutrients alone don't really go into bone building mode unless there's demand on the bones. That means load. Likewise, even with strong bones, we don't stay upright if our movement is compromised by various aches and pains.
A new research survey on non-invasive approaches to bone building puts these points together in a really nice review called "Physical approach for prevention and treatment of osteoporosis" The nice thing is it's free.
Summary: Here's a summary of the approaches that look good for building up bone mineral density:
BONE BUILDING
Resistance training - that's good but it's also site specific. In other words, lower body work helps the lower body (hip/pelvis); upper body work helps the upper body (including the critical spine).
Impact Training - this is stop and start and "odd angle" activities like soccer or squash (not running so much), but also for the more frail, even dancing and ball games have been proposed as ways to help keep demand up on bones.
Combinations. Meta analysis of research suggests that the best approach, unsurprisingly is a mixed approach of resistance training and impact training. Fortunately such practice can be fun and have bone building effect.
Vibration. the next time someone pooh poohs force plates, you might want to suggest that they've been shown - repeatedly - to help build up bone. It's not a HUGE gain, but it could be an excellent modality for the initially infirm:
BALNANCE - Physical and Hormonal
 T'ai Chi - does nothing for bone building at all, BUT helps get on with movement and balance and the breathing can help destress, so hormonally very helpful in supporting staying safe. Research has mainly focused on T'ai Chi for these effects, but it might be interesting to consider that other approaches that emphasize mobility, balance, de-stressing, and the whole sensory motor apparatus might not benefit here too?
T'ai Chi - does nothing for bone building at all, BUT helps get on with movement and balance and the breathing can help destress, so hormonally very helpful in supporting staying safe. Research has mainly focused on T'ai Chi for these effects, but it might be interesting to consider that other approaches that emphasize mobility, balance, de-stressing, and the whole sensory motor apparatus might not benefit here too?
BUILDING & REPAIR
New & Approved. The review also considers several other forms of "physical agents" like Low Intensity Pulsed Ultrasound (LIPUS) that has been shown to stimulate bone repair. Electrical stimulation has also now been approved by the FDA for "bone repair."
Experimental. Pulsed electro magnetic fields (PEMF) is a newer approach, nothing conclusive there yet. Low Level Laser Therapy is also being trialed in animal models, but again nothing yet in human studies.
Role for Movement Practice & Assessment?
Where we seem to be at is that concern about bone mineral density has two components: first is to ensure practices for maintianing and building BMD, but second is the development of practices to help people feel stable and mobile rather than vulnerable to falls - improving range of motion, visual accuity and balance. It's not just Range of Motion - thought that's important - it's the whole sensory-motor awareness package.
It doesn't matter if we're younger or older - we can have issues with our movement that can compromise our ability to respond with agility to a tricky situation. The entire functional movement screen program is based on the premise that there's no point building strength on top of dysfunction, hence the screen for movement issues.
 But likewise, we can have issues with our balance or visual accuity or our brains ability to perceive our selves clearly in motion. Indeed, i've written quite a bit about the benefit of just kicking off our restrictive shoes to get more info to the brain about where we are in space, and how doing so has pretty big benefits for movement and also feel of one's own mobility (as the feet move more and better, it seems so do other joints).
But likewise, we can have issues with our balance or visual accuity or our brains ability to perceive our selves clearly in motion. Indeed, i've written quite a bit about the benefit of just kicking off our restrictive shoes to get more info to the brain about where we are in space, and how doing so has pretty big benefits for movement and also feel of one's own mobility (as the feet move more and better, it seems so do other joints).
So it seems pretty basic that as part of our quest for better bone health, a related quest for optimizing our body's ability to move in space is pretty important. I've said before, this awareness development is part of why i like I-Phase so much: it's prepping the body for the Real.
In other words, as we build better bones, there's a real benefit in openning up our body's awareness of itself in space, and simultaneously, it's ability to respond better to what's happening.
Simple example: better range of motion combined with better practice of movement into multiple positions, and better balance and visual processing means the brain has more knowledge about its being able to Zig rather than having to Zag around that wet spot on the floor, and thus, us not going for a tumble.
Stronger bones PLUS less risk of falling in the first place (and not being able to get up) - that seems to be more a complete package.
Conclusion: Why is osteoperosis such the women's issue?
One advantage that guys have is the size of their muscles puts more load on their bones so that the bones are under more demand. More demand on the bones, more continued adapting to load.
Women have not been encouraged to do as much manual labour or high resistance workouts as guys.
Similarly our formal worlds are increasingly desk bound, so less movement is part of our daily lives. As we age, this decrease in multi-plane motion seems to increase. Let us say phooey to this increasingly restricted mode of being.
It will be interesting to see as the culture shifts towards it being ok for gals to work out, and as muscle tissue can be built up at any age, that perhaps hip and related fractures will become a fate of a by-gone age.
Citation:
Related Resources
A new research survey on non-invasive approaches to bone building puts these points together in a really nice review called "Physical approach for prevention and treatment of osteoporosis" The nice thing is it's free.
Summary: Here's a summary of the approaches that look good for building up bone mineral density:
BONE BUILDING
Resistance training - that's good but it's also site specific. In other words, lower body work helps the lower body (hip/pelvis); upper body work helps the upper body (including the critical spine).
Impact Training - this is stop and start and "odd angle" activities like soccer or squash (not running so much), but also for the more frail, even dancing and ball games have been proposed as ways to help keep demand up on bones.
Combinations. Meta analysis of research suggests that the best approach, unsurprisingly is a mixed approach of resistance training and impact training. Fortunately such practice can be fun and have bone building effect.
Vibration. the next time someone pooh poohs force plates, you might want to suggest that they've been shown - repeatedly - to help build up bone. It's not a HUGE gain, but it could be an excellent modality for the initially infirm:
A 1-year prospective, randomized, double-blind, and placebo-controlled trial of postmenopausal women demonstrated that 20 minutes of a low-level vibration applied during quiet standing can effectively inhibit bone loss in the spine and femur. Placebo subjects lost 2.13% in the femoral neck over 1 year, whereas treatment was associated with a gain of 0.04%, reflecting a 2.17% relative benefit of treatment. In the spine, the 1.6% decrease observed over 1 year in the placebo group was reduced to a 0.10% loss in the active group, indicating a 1.5% relative benefit of treatment (40).
BALNANCE - Physical and Hormonal
T'ai Chi - does nothing for bone building at all, BUT helps get on with movement and balance and the breathing can help destress, so hormonally very helpful in supporting staying safe. Research has mainly focused on T'ai Chi for these effects, but it might be interesting to consider that other approaches that emphasize mobility, balance, de-stressing, and the whole sensory motor apparatus might not benefit here too?BUILDING & REPAIR
New & Approved. The review also considers several other forms of "physical agents" like Low Intensity Pulsed Ultrasound (LIPUS) that has been shown to stimulate bone repair. Electrical stimulation has also now been approved by the FDA for "bone repair."
Experimental. Pulsed electro magnetic fields (PEMF) is a newer approach, nothing conclusive there yet. Low Level Laser Therapy is also being trialed in animal models, but again nothing yet in human studies.
Role for Movement Practice & Assessment?
Where we seem to be at is that concern about bone mineral density has two components: first is to ensure practices for maintianing and building BMD, but second is the development of practices to help people feel stable and mobile rather than vulnerable to falls - improving range of motion, visual accuity and balance. It's not just Range of Motion - thought that's important - it's the whole sensory-motor awareness package.
It doesn't matter if we're younger or older - we can have issues with our movement that can compromise our ability to respond with agility to a tricky situation. The entire functional movement screen program is based on the premise that there's no point building strength on top of dysfunction, hence the screen for movement issues.
 But likewise, we can have issues with our balance or visual accuity or our brains ability to perceive our selves clearly in motion. Indeed, i've written quite a bit about the benefit of just kicking off our restrictive shoes to get more info to the brain about where we are in space, and how doing so has pretty big benefits for movement and also feel of one's own mobility (as the feet move more and better, it seems so do other joints).
But likewise, we can have issues with our balance or visual accuity or our brains ability to perceive our selves clearly in motion. Indeed, i've written quite a bit about the benefit of just kicking off our restrictive shoes to get more info to the brain about where we are in space, and how doing so has pretty big benefits for movement and also feel of one's own mobility (as the feet move more and better, it seems so do other joints). So it seems pretty basic that as part of our quest for better bone health, a related quest for optimizing our body's ability to move in space is pretty important. I've said before, this awareness development is part of why i like I-Phase so much: it's prepping the body for the Real.
In other words, as we build better bones, there's a real benefit in openning up our body's awareness of itself in space, and simultaneously, it's ability to respond better to what's happening.
Simple example: better range of motion combined with better practice of movement into multiple positions, and better balance and visual processing means the brain has more knowledge about its being able to Zig rather than having to Zag around that wet spot on the floor, and thus, us not going for a tumble.
Stronger bones PLUS less risk of falling in the first place (and not being able to get up) - that seems to be more a complete package.
Conclusion: Why is osteoperosis such the women's issue?
One advantage that guys have is the size of their muscles puts more load on their bones so that the bones are under more demand. More demand on the bones, more continued adapting to load.
Women have not been encouraged to do as much manual labour or high resistance workouts as guys.
Similarly our formal worlds are increasingly desk bound, so less movement is part of our daily lives. As we age, this decrease in multi-plane motion seems to increase. Let us say phooey to this increasingly restricted mode of being.
It will be interesting to see as the culture shifts towards it being ok for gals to work out, and as muscle tissue can be built up at any age, that perhaps hip and related fractures will become a fate of a by-gone age.
Citation:
Lirani-Galvão, A., Lazaretti-Castro, M. (2010). Physical approach for prevention and treatment of osteoporosis Arquivos Brasileiros de Endocrinologia & Metabologia, 54 (2) DOI: 10.1590/S0004-27302010000200013
Related Resources
- What is z-health
- ck-fms - what is it
- the other side of the gym: developing sensory motor performance
- DO YOUR SHOES PASS THE TWIST TEST?
Saturday, May 22, 2010
Real Chocolate Cake: how to make it? with 100% REAL cacao of course- "100% or go home"
Follow @mcphoo
Tweet
Chocolate is good for us. Really. It's got all sorts of health things going for it - particularly when it's as close to its pure cacao form as possible (here's a detailed overview of why). I really enjoy a square of Lindt 85% or 99% cacao bar for a taste treat in the evening - one of the advantages is that that's pretty much all a person wants: one square - very satisfying.
 Recently i was welcomed to the next level of cacao bliss: baking with the stuff - pure 100% cacao. Oh wow. No offense to Baker's Chocolate, but my word, the taste difference of using real cacao is so incredible, my guess is once you try it you won't want anything else. Let me help you prove this to yourself.
Recently i was welcomed to the next level of cacao bliss: baking with the stuff - pure 100% cacao. Oh wow. No offense to Baker's Chocolate, but my word, the taste difference of using real cacao is so incredible, my guess is once you try it you won't want anything else. Let me help you prove this to yourself.
In the UK, there is a company called Willie's cacao (no affiliation, and i'm sorry about the annoying flash site) that sells cacao in these chunky cylynders that's ideal for baking and cooking.
The chocolate itself supposedly comes from the owner's farm on the Other Side of the pond and to the south, while it's processed in the UK on 100 year old chocolate making equipment. Not sure how that makes it taste better, but oh well.
The point is that one can swap out cooking chocolate like bakers from any recipe, put this stuff in instead and suddenly the taste experience just goes up - exponentially.
By way of example, if you would really like to give this taste experience a chance, here's avariant on an old but delicious Baker's Chocolate Cake Recipe, that really, if you do this swap, you'll be well, on another plane of desert experience.
This is not a recipe that is shy of real serious ingredients. Use them; don't skip on making anything less fat than is called for. You're doing this because you know you can make this, freeze it and take out a piece from time to time. Seriously. IT's almost better (like Sara Lee cake if made by gods) post frozen.
Ok Here we go:
classic german chocolate cake (history of german choc. cake)
Prep Time: 40 minutes. Bake Time 30 minutes
a whole cylynder of the Peruvian Black Willie's Cacao (180g)
1,1/4 cup butter
2 1/2 cup granulated sugar (prefer organic castor sugar or nat. unrefined cane sugar)
6 eggs
2 cups all purpose flour
1tsp baking soda
1 cup buttermilk - no skimping
Coconut Pecan Icing
1 cup evaporated milk
1 cup granulated sugar
3 slightly beaten egg yolks
1/2 cup butter
1 tsp vanilla - real vanilla, please
1 1/2 cup schreded coconut - try to get flakes, and not fresh - that's too moist
1 cup chopped pecans
Cake:
1. nuke the chocoalate and butter in a big nuker bowl on high for about 2 minutes. stui until choc. is completely melted.
2. stir in sugar until well belnded . Add eggs one at a time, mix well. Beat in flour and baking soda alternately with buttermilk until smooth. Pour into bunt pan (here we break with tradition of the cake pans)
3. Bake in preheated 350F oven for 1hr10mi. Use the toothpick test if you wish to check readiness. for departure from over. Cool on a rack.

Icing:
Combine milk, sugar, egg yolks, butter and vanilla in saucepan. Bring to a BOIL. COok and stir over medium heat about 8 to 10 minutes or until golden. Remove from heat. Stir in cocnut and nuts. Cool, spread frosting over top of cake.

Now that last instruction is tricky. You'll have frosting left over most like which is fine as it can be used on the side by guests (or yourself depnding on mood) to add more like a spread should they wish - or decline and pretend to be healthier for declining extra icing.
Experience
Well what can i tell you? it's delicious the first day; it matures and tastes richer the seond, and post freezing, it's the gift that keeps on giving.
This is not a cheap cake - the chocolate alone is 6quid; ya'll know how much butter and high grade eggs cost, but really quality ingredients do make a difference. And if food is something you love, and for something that will be available for some time unless you go all gluttonish on it, it will be a wonderful experience for yourself, or you and the folks you love.
I'd be keen to hear if you can't get Willie's in your country, what options you've found for Cooking Cacao.
mc Tweet Follow @begin2dig

In the UK, there is a company called Willie's cacao (no affiliation, and i'm sorry about the annoying flash site) that sells cacao in these chunky cylynders that's ideal for baking and cooking.
The chocolate itself supposedly comes from the owner's farm on the Other Side of the pond and to the south, while it's processed in the UK on 100 year old chocolate making equipment. Not sure how that makes it taste better, but oh well.
The point is that one can swap out cooking chocolate like bakers from any recipe, put this stuff in instead and suddenly the taste experience just goes up - exponentially.
By way of example, if you would really like to give this taste experience a chance, here's avariant on an old but delicious Baker's Chocolate Cake Recipe, that really, if you do this swap, you'll be well, on another plane of desert experience.
This is not a recipe that is shy of real serious ingredients. Use them; don't skip on making anything less fat than is called for. You're doing this because you know you can make this, freeze it and take out a piece from time to time. Seriously. IT's almost better (like Sara Lee cake if made by gods) post frozen.
Ok Here we go:
classic german chocolate cake (history of german choc. cake)
Prep Time: 40 minutes. Bake Time 30 minutes
a whole cylynder of the Peruvian Black Willie's Cacao (180g)
1,1/4 cup butter
2 1/2 cup granulated sugar (prefer organic castor sugar or nat. unrefined cane sugar)
6 eggs
2 cups all purpose flour
1tsp baking soda
1 cup buttermilk - no skimping
Coconut Pecan Icing
1 cup evaporated milk
1 cup granulated sugar
3 slightly beaten egg yolks
1/2 cup butter
1 tsp vanilla - real vanilla, please
1 1/2 cup schreded coconut - try to get flakes, and not fresh - that's too moist
1 cup chopped pecans
Cake:
1. nuke the chocoalate and butter in a big nuker bowl on high for about 2 minutes. stui until choc. is completely melted.
2. stir in sugar until well belnded . Add eggs one at a time, mix well. Beat in flour and baking soda alternately with buttermilk until smooth. Pour into bunt pan (here we break with tradition of the cake pans)
3. Bake in preheated 350F oven for 1hr10mi. Use the toothpick test if you wish to check readiness. for departure from over. Cool on a rack.

cooling cake on rack
Icing:
Combine milk, sugar, egg yolks, butter and vanilla in saucepan. Bring to a BOIL. COok and stir over medium heat about 8 to 10 minutes or until golden. Remove from heat. Stir in cocnut and nuts. Cool, spread frosting over top of cake.

exemplar cacao enriched cake, dressed for festive occaision.
Experience
Well what can i tell you? it's delicious the first day; it matures and tastes richer the seond, and post freezing, it's the gift that keeps on giving.
This is not a cheap cake - the chocolate alone is 6quid; ya'll know how much butter and high grade eggs cost, but really quality ingredients do make a difference. And if food is something you love, and for something that will be available for some time unless you go all gluttonish on it, it will be a wonderful experience for yourself, or you and the folks you love.
I'd be keen to hear if you can't get Willie's in your country, what options you've found for Cooking Cacao.
mc Tweet Follow @begin2dig
Thursday, May 20, 2010
Should i do this next set? Pre-cognitive Fatigue Testing
Follow @mcphoo
Tweet
In a work out, how can you tell if you're sufficiently recovered to do another set or if your *nervous system* is too fried to try? How can we get a measure that you can't inadvertently cheat cuz we're so keen to get in our sets, we might be willing to kid ourselves?
Range of motion checks which are used in Z-Heatlh, and are becoming popular in approaches like Gym Movement (overview) are grand for many things, but they're cognitive: we can push a toe touch a little more or less between efforts; we need to think about whether this last test compares with this current test. That's fine, but sometimes, we might want something where we really don't have to think about it - especially when already pushing ourselves. We want something that's precognitve. Balance testing is one way to get at this nervous-system response.
 Simple practice: before starting a set, stand on one foot, turn head sharply to the left; notice stability, then turn head sharply to the right; notice stability. The spin MUST be fast to get the fluid in the inner ear moving.
Simple practice: before starting a set, stand on one foot, turn head sharply to the left; notice stability, then turn head sharply to the right; notice stability. The spin MUST be fast to get the fluid in the inner ear moving.
Now, do the same test with the other foot.
Repeat the whole sequence with eyes closed.
The important thing here is to benchmark performance - if standing on the left foot, ya kinda fall over with your eyes closed when turning right fast, that's ok; just make a note to self of how you performed.
Now go for your sets. (Thanks to tom robinson posing for the above demo)
Ready Ready? If you have a question mark about the next set planned, redo your balance tests right after your last set. If you're wobbly in new ways from the baseline, you know that you are NOT ready to continue another set - well, your nervous system isn't.
The key now is to wait your usual reovery time, and retest. Are you back to at least where you were when you came into the gym? No? wait longer. Retest. if by five minutes you're still unhinged, bag it.
Feedback. I've been using this approach for everything from skipping sets to pressing sets, and the results are better quality sets and better recovery.
Last night my workout said i had two more sets of presses and pistols to go, but my recovery test was still wobbly, so i bagged the sets. On another occaision, between skipping sets i was all over wobbly mid workout; waited to recover, and each time after that i checked balance i was way way more stable, and had some of the best sets i've had. Just from that mid-set breather.
I like this check because it's not debatable: if i've nearly fallen over in a closed eye test where i was stable before, that's telling me something about my sensory-motor capabilities at this moment. Why would i want to add load to that?
Resources for More Like This: This test and many many more are available on a new Z-Health DVD Mini Course: Essentials of Elite Performance. It's an actual course - what they're calling a mini-course, based on their 3day Essentials of Elite Performance workshop (overviewed here).
 If you can't get to the workshop (calendar here), or just want to get going now on skills like these now, the DVD course has a whole TON of sensory-motor self-assessments and tune ups.
If you can't get to the workshop (calendar here), or just want to get going now on skills like these now, the DVD course has a whole TON of sensory-motor self-assessments and tune ups.
Please check the site for the full list of Good Things covered on the 3DVD/6.5 hours course.
And here's a cool thing: if you get the DVD, are smitten with the material, so you sign up for the full Essentials workshop or R-phase Z-Health course, you'll get 100 bucks off the tuition of that course. That's nice.
Anyway, i'd be keen to hear from you on how you find the balance test. Talking with some z-health master trainers, i've been reminded that different tests work differently in different contexts. If you're doing something where you're highly experienced, the balance test mayn't show fatigue as well as say a peripheral vision or range of motion test - it depends on the individual. Which is what makes this particualr DVD set cool: it provides a range of self-tests, as well as the rationales behind them, so we have good resources for our self-diagnostic tool box that are clear, unambiguous and repeatable.
But to repeat - please let me know how this one works for you and where you used it in what routine.
best
mc
Related Resources
Range of motion checks which are used in Z-Heatlh, and are becoming popular in approaches like Gym Movement (overview) are grand for many things, but they're cognitive: we can push a toe touch a little more or less between efforts; we need to think about whether this last test compares with this current test. That's fine, but sometimes, we might want something where we really don't have to think about it - especially when already pushing ourselves. We want something that's precognitve. Balance testing is one way to get at this nervous-system response.

Now, do the same test with the other foot.
Repeat the whole sequence with eyes closed.
The important thing here is to benchmark performance - if standing on the left foot, ya kinda fall over with your eyes closed when turning right fast, that's ok; just make a note to self of how you performed.
Now go for your sets. (Thanks to tom robinson posing for the above demo)
Ready Ready? If you have a question mark about the next set planned, redo your balance tests right after your last set. If you're wobbly in new ways from the baseline, you know that you are NOT ready to continue another set - well, your nervous system isn't.
The key now is to wait your usual reovery time, and retest. Are you back to at least where you were when you came into the gym? No? wait longer. Retest. if by five minutes you're still unhinged, bag it.
Feedback. I've been using this approach for everything from skipping sets to pressing sets, and the results are better quality sets and better recovery.
Last night my workout said i had two more sets of presses and pistols to go, but my recovery test was still wobbly, so i bagged the sets. On another occaision, between skipping sets i was all over wobbly mid workout; waited to recover, and each time after that i checked balance i was way way more stable, and had some of the best sets i've had. Just from that mid-set breather.
I like this check because it's not debatable: if i've nearly fallen over in a closed eye test where i was stable before, that's telling me something about my sensory-motor capabilities at this moment. Why would i want to add load to that?
Resources for More Like This: This test and many many more are available on a new Z-Health DVD Mini Course: Essentials of Elite Performance. It's an actual course - what they're calling a mini-course, based on their 3day Essentials of Elite Performance workshop (overviewed here).
If you can't get to the workshop (calendar here), or just want to get going now on skills like these now, the DVD course has a whole TON of sensory-motor self-assessments and tune ups.Please check the site for the full list of Good Things covered on the 3DVD/6.5 hours course.
And here's a cool thing: if you get the DVD, are smitten with the material, so you sign up for the full Essentials workshop or R-phase Z-Health course, you'll get 100 bucks off the tuition of that course. That's nice.
Anyway, i'd be keen to hear from you on how you find the balance test. Talking with some z-health master trainers, i've been reminded that different tests work differently in different contexts. If you're doing something where you're highly experienced, the balance test mayn't show fatigue as well as say a peripheral vision or range of motion test - it depends on the individual. Which is what makes this particualr DVD set cool: it provides a range of self-tests, as well as the rationales behind them, so we have good resources for our self-diagnostic tool box that are clear, unambiguous and repeatable.
But to repeat - please let me know how this one works for you and where you used it in what routine.
best
mc
Related Resources
- The other Side of the Gym: sensory motor tuning
- How's your Eye Fitness?
- Eye position for Rowing performance
- Efficient Movement - coming back to the Kettlebell Front Squat
- Arthrokinetic Reflex and the KB swing
begin2dig (b2d) on Facebook
Tweet
Follow @begin2dig
Excessive Daytime Sleepiness - Can be a Big Issue predictor.
Follow @mcphoo
Tweet
Sleep is so important. Sleepiness during the day may likewise be a really critical health marker. Sleepiness itself is usually taken as a sign that we just didn't get enough kip. Sometimes figuring out why is easy, and we can fix it; sometimes figuring out why is a little more elusive, and getting some knowledgable help is a great idea. Note: if you're considering seeing a trainer or coach, find out from them what kind of HISTORY they take about your wellbeing. If there's nothing in there about the qualities of what i've been calling our H2 Ratio, you may want to have a chat with someone else.
We know that chronic sleepiness in"older adults", is a marker of potential heart issues and mortality risk. It also seems to show up some specific correlations around mental and physical well being too.
While doing some work on sleep in our lab project on personal wellbeing tracking, i came across the following studies on EDS (excessive daytime sleepiness). The first is EDS as a marker of risk for "older adults"
Why folks feel sleepy during the day we know may stem from multiple causes. Nutrition issues, pain, breathing difficulties, lack of movement during the day, medication, sleep disorders. But it seems one of the highlights from this article is that it's REALLY IMPORTANT that if one is chronically sleepy, it's more than a good idea to check in about what might be causing that sleepiness and get it addressed.
Likewise, a more recent study looked at quality of life responses across ethnic groups relative to sleep disturbances/EDS. Here's what they report.
So as with the "older adult" study, sleep issues may be showing up as a consequence of related factors. THat's not a particular surprise. What we do know, however, is that crappy sleep in itself - that can show up as excessive daytime sleepiness too - is not good for health. We need quality z's.
A recent survey of evaluation approaches shows there are LOTS of ways to check in with a person about possible causes and developing a strategy towards getting better sleep. And, if you're interested more generally in what sleep is, and what some known sleep issues are, there's a nice current overview - free paper - called simply "Overview of sleep & sleep disorders."
Sleep Practice Feedback. In my group, we're doing research looking at the role awareness may play in wellbeing, health, quality of life. One of the devices we're using as a feed for the data is the Zeo. I've written about this before with a two part interview with Stephen Fabregas, sleep researcher, at Zeo. I'm also in the throes of prepping a review of using the device.
[EDIT - 2013: unfortunately the following kit is no longer available as zeo has closed down. THere are simple sleep monitors in commercial hardware like FitBit and Jawbone UP and also free actigarphy monitors on many phone platforms: these at least give an indication of time in bed/asleep and time restless. it's all about trends...]
Early summary: i really like it, and yes it's helped modify my behaviour to get better quality sleep. Why? because i can *see* it - my sleep cycles - i want to understand why i had less deep sleep or what's going on with low REM compared to how i usually sleep. What's different? Pretty simply it gives me a way to help make more grounded sense of how i'm doing. And it's making a difference.
There's also a sleep coach program that i'm just getting into, so that's why the review is not out yet - i want to see what that does, too. But even without the sleep coach, this device, compared with all the sleep info on the site, has been making a real difference to my perceived well being.
If you're interested, Zeo is offering a 10dollar off/free shipping deal with a coupon (here's the link). As said, i like it. I'm learning a lot. And am using it more than i do a heart rate monitor right now perhaps because this is such a new area of investigation for me.
 Now, getting a zeo is not a replacement at all if one is suffering from excessive daytime sleepiness or related sleep issues in sitting down with a health pro to find out what may be going on with one's sleep - if there is some disease or drug or related Big Deal happening that requires attention. And sleep, as stephan said in the interviews, is SO crucial, and as the above research shows it's critical to get on top of it.
Now, getting a zeo is not a replacement at all if one is suffering from excessive daytime sleepiness or related sleep issues in sitting down with a health pro to find out what may be going on with one's sleep - if there is some disease or drug or related Big Deal happening that requires attention. And sleep, as stephan said in the interviews, is SO crucial, and as the above research shows it's critical to get on top of it.
What a zeo can do is reflect back, pretty clearly, if those strategies are working, and if so, how well. That wee display can also help keep us honest about our practice, and help us tune that practice. So it's no replacement for real counciling (nor is it designed to be) around a chronic issue, but it's a great way to help dial in and feedback the practice.
For instance, some of the quesitons i've had are: all things being equal, does timing of exercise in the evening REALLY effect my sleep quality? Does doing two split workouts a day do better than one? Can i really see any difference on fasting or better quality eating days? Very personal tuning to be sure, but it wasn't really possible to ask these quesitons previously as i had no real, clear way of correlating sleep with these practices. There's a section on the site "for health pros" that lists the research on this puppy.
Summary: Daytime sleepiness especially if it starts to become a pattern is NOT a good thing. It's associated with everything from poor mental health to, well, death. So, it's very much worth getting sleep quality up (and daytime sleepiness down). Sleepiness during the day, especially in older adults, seems to be a strong marker of a potential issue.
If general healthy sleep practices aren't working, checking in with a health professional like one's GP about what factors may be influencing it, and getting on top of it, are really important. It's awful to have health issues already where more will be amplified by poor sleep. A vicious cycle that needs to be broken. A sleep monitor tool in these cases to give good feedback on how well strategies, once they've been developed, are working.
Absolutely check with your GP; if you are not being physical yet, getting one with starting movement can be a HUGE boon. Here's an overview of getting some Time under Movement
If you are already moving and experiencing sleepiness, working with a qualified practitioner /coach who can look at your movement, nutrition, sleep and related is a Good Thing. I personally work with folks in consultation with their GP's assessments. They go great together.
But main takeaway: chronic daytime sleepiness - it's our bodies talking to us in a BIG WAY to say something needs to change. Seek help in figuring out what things to tune and how. You'll love how you feel.
Citations
We know that chronic sleepiness in"older adults", is a marker of potential heart issues and mortality risk. It also seems to show up some specific correlations around mental and physical well being too.
While doing some work on sleep in our lab project on personal wellbeing tracking, i came across the following studies on EDS (excessive daytime sleepiness). The first is EDS as a marker of risk for "older adults"
J Am Geriatr Soc. 2000 Feb;48(2):115-23.
Daytime sleepiness predicts mortality and cardiovascular disease in older adults. The Cardiovascular Health Study Research Group.
Newman AB, Spiekerman CF, Enright P, Lefkowitz D, Manolio T, Reynolds CF, Robbins J. University of Pittsburgh, Pennsylvania 15213, USA.
INTRODUCTION: As part of the baseline examination in the Cardiovascular Health Study, sleep disturbance symptoms including snoring and daytime sleepiness, were assessed as potential risk factors or precipitants of cardiovascular disease (CVD). Because of the association of sleep disturbance with poorer health and the possible associations of sleep apnea with CVD, we hypothesized that those with poorer sleep or daytime sleepiness may be at increased risk of mortality or incident CVD. SETTING: Participants (n = 5888) were recruited in 1989, with an additional minority cohort recruited in 1993, in four US communities for a cohort study designed to evaluate risk factors for cardiovascular disease. METHODS: An interview-administered questionnaire regarding health and sleep habits with ongoing ascertainment of total mortality and cardiovascular disease morbidity and mortality, including total CVD morbidity and mortality, incident myocardial infarction, and congestive heart failure. RESULTS: Daytime sleepiness was the only sleep symptom that was significantly associated with mortality in both men and women. The unadjusted hazard ratio was 2.12 (1.66, 2.72) in women and 1.40 (1.12, 1.73) in men. Men who reported difficulty falling asleep also had an increased mortality rate (HR = 1.43 (1.14, 1.80)) which was not seen in women. The risks were attenuated with adjustment for age but remained significant for daytime sleepiness in women (HR = 1.82 (1.42, 2.34)) and for difficulty falling asleep in men. (HR = 1.29 (1.03, 1.63)). Frequent awakenings, early morning awakening, and snoring were not associated with a significantly increased risk of mortality in these older men and women. Crude event rates were evaluated for total incident cardiovascular morbidity and mortality, incident myocardial infarction, and incident congestive heart failure (CHF). Incident CVD rates were higher in both men and women with daytime sleepiness. The aged adjusted HR was 1.35 (95% CI = 1.03, 1.76) in men and was 1.66 (95% CI = 1.28, 2.16) in women. Incident CVD was not higher in those with any other sleep disturbance including snoring. The risk of CVD events associated with daytime sleepiness was attenuated but remained significant in women after adjustment for age. Incident myocardial infarction (MI) rates were also higher in women with daytime sleepiness but were not significantly higher in men. Incident CHF rates were increased in both men and women with daytime sleepiness. In men, the age adjusted HR was 1.49 (95% CI, 1.12- 1.98) and in women, was 2.21 (95% CI, 1.64-2.98). Women reporting both daytime sleepiness and frequent awakening had a hazard ratio of 2.34 (95% CI, 1.66-3.29) for incident CHF compared with those with daytime sleepiness but without frequent awakening. This interaction was not found in men. CONCLUSIONS: In this study, daytime sleepiness was the only sleep disturbance symptom that was associated with mortality, incident CVD morbidity and mortality, MI, and CHF. These findings were stronger in women than men, i.e., the associations persisted for mortality, CVD, and CHF in women after adjustment for age and other factors. Thus, a report of daytime sleepiness identifies older adults at increased risk for total and cardiovascular mortality, and is an independent risk factor in women.The big deal here is the end of this abstract - the signs being described have much the ring of metabolic syndrome to them, don't they?
Why folks feel sleepy during the day we know may stem from multiple causes. Nutrition issues, pain, breathing difficulties, lack of movement during the day, medication, sleep disorders. But it seems one of the highlights from this article is that it's REALLY IMPORTANT that if one is chronically sleepy, it's more than a good idea to check in about what might be causing that sleepiness and get it addressed.
Likewise, a more recent study looked at quality of life responses across ethnic groups relative to sleep disturbances/EDS. Here's what they report.
J Clin Sleep Med. 2010 Apr 15;6(2):176-83.What the study suggests is that sleep disturbances and results like excessive daytime sleepiness (25% of the total cohort of over 5000 participants) seem to correlate with different effects on mental/physical health relative to (a) US Norms and (b) ethnicity. A key conclusion, however, is that, while these results are indicative, they may be part of "comorbid health conditions" - in other words, the sleep related problems and their associated responses may be part of a package of issues.
Sleep disturbances, quality of life, and ethnicity: the Sleep Heart Health Study.
Baldwin CM, Ervin AM, Mays MZ, Robbins J, Shafazand S, Walsleben J, Weaver T.
Arizona State University College of Nursing and Health Innovation, Phoenix, AZ 85004, USA. carol.baldwin@asu.edu
Abstract
STUDY OBJECTIVES: To compare health-related quality of life (HR-QOL) across subgroups defined by sleep disturbances and ethnicity. METHODS: Men (47%) and women (53%) Sleep Heart Health Study participants age 40 and older (N = 5237) underwent overnight polysomnography and completed self-report questionnaires on symptoms of sleep disturbances. The physical and mental composite scales (PCS and MCS) of the Medical Outcomes Study 36-item short form survey assessed HR-QOL and were compared to sleep data. RESULTS: Participants self-identified as Caucasian/White (n = 4482, 86%), African American/Black (n = 490, 9%), or Hispanic/Mexican American (n = 265, 5%). The prevalence of obstructive sleep apnea (OSA) was 17%, frequent snoring was 34%, difficulty initiating or maintaining sleep (DIMS; insomnia symptoms) was 30%, and excessive daytime sleepiness (EDS) was 25%. African American participants with frequent snoring, insomnia symptoms, or EDS had significantly poorer physical health compared to Caucasians (p < 0.001). Hispanics with frequent snoring, insomnia symptoms, or EDS had significantly poorer mental health than Caucasian participants (p <0.001). Neither PCS nor MCS scores differed significantly across ethnic subgroups for participants with moderate to severe OSA (respiratory disturbance index > 15, 4% desaturation). CONCLUSIONS: Across ethnic/racial subgroups, sleep disturbances are associated with worse physical and better mental HR-QOL than the U.S. norm, but this relationship may be moderated by comorbid health conditions. This study replicates and extends prior research indicating differences among minority and non-minority participants and highlights the need for future studies of sleep disturbances with larger samples of minorities that control for comorbid health conditions.
So as with the "older adult" study, sleep issues may be showing up as a consequence of related factors. THat's not a particular surprise. What we do know, however, is that crappy sleep in itself - that can show up as excessive daytime sleepiness too - is not good for health. We need quality z's.
A recent survey of evaluation approaches shows there are LOTS of ways to check in with a person about possible causes and developing a strategy towards getting better sleep. And, if you're interested more generally in what sleep is, and what some known sleep issues are, there's a nice current overview - free paper - called simply "Overview of sleep & sleep disorders."
Sleep Practice Feedback. In my group, we're doing research looking at the role awareness may play in wellbeing, health, quality of life. One of the devices we're using as a feed for the data is the Zeo. I've written about this before with a two part interview with Stephen Fabregas, sleep researcher, at Zeo. I'm also in the throes of prepping a review of using the device.
[EDIT - 2013: unfortunately the following kit is no longer available as zeo has closed down. THere are simple sleep monitors in commercial hardware like FitBit and Jawbone UP and also free actigarphy monitors on many phone platforms: these at least give an indication of time in bed/asleep and time restless. it's all about trends...]
Early summary: i really like it, and yes it's helped modify my behaviour to get better quality sleep. Why? because i can *see* it - my sleep cycles - i want to understand why i had less deep sleep or what's going on with low REM compared to how i usually sleep. What's different? Pretty simply it gives me a way to help make more grounded sense of how i'm doing. And it's making a difference.
There's also a sleep coach program that i'm just getting into, so that's why the review is not out yet - i want to see what that does, too. But even without the sleep coach, this device, compared with all the sleep info on the site, has been making a real difference to my perceived well being.
If you're interested, Zeo is offering a 10dollar off/free shipping deal with a coupon (here's the link). As said, i like it. I'm learning a lot. And am using it more than i do a heart rate monitor right now perhaps because this is such a new area of investigation for me.
Now, getting a zeo is not a replacement at all if one is suffering from excessive daytime sleepiness or related sleep issues in sitting down with a health pro to find out what may be going on with one's sleep - if there is some disease or drug or related Big Deal happening that requires attention. And sleep, as stephan said in the interviews, is SO crucial, and as the above research shows it's critical to get on top of it.What a zeo can do is reflect back, pretty clearly, if those strategies are working, and if so, how well. That wee display can also help keep us honest about our practice, and help us tune that practice. So it's no replacement for real counciling (nor is it designed to be) around a chronic issue, but it's a great way to help dial in and feedback the practice.
For instance, some of the quesitons i've had are: all things being equal, does timing of exercise in the evening REALLY effect my sleep quality? Does doing two split workouts a day do better than one? Can i really see any difference on fasting or better quality eating days? Very personal tuning to be sure, but it wasn't really possible to ask these quesitons previously as i had no real, clear way of correlating sleep with these practices. There's a section on the site "for health pros" that lists the research on this puppy.
Summary: Daytime sleepiness especially if it starts to become a pattern is NOT a good thing. It's associated with everything from poor mental health to, well, death. So, it's very much worth getting sleep quality up (and daytime sleepiness down). Sleepiness during the day, especially in older adults, seems to be a strong marker of a potential issue.
If general healthy sleep practices aren't working, checking in with a health professional like one's GP about what factors may be influencing it, and getting on top of it, are really important. It's awful to have health issues already where more will be amplified by poor sleep. A vicious cycle that needs to be broken. A sleep monitor tool in these cases to give good feedback on how well strategies, once they've been developed, are working.
Absolutely check with your GP; if you are not being physical yet, getting one with starting movement can be a HUGE boon. Here's an overview of getting some Time under Movement
If you are already moving and experiencing sleepiness, working with a qualified practitioner /coach who can look at your movement, nutrition, sleep and related is a Good Thing. I personally work with folks in consultation with their GP's assessments. They go great together.
But main takeaway: chronic daytime sleepiness - it's our bodies talking to us in a BIG WAY to say something needs to change. Seek help in figuring out what things to tune and how. You'll love how you feel.
begin2dig (b2d) on Facebook
Citations
Tweet Follow @begin2dig
Newman AB, Spiekerman CF, Enright P, Lefkowitz D, Manolio T, Reynolds CF, & Robbins J (2000). Daytime sleepiness predicts mortality and cardiovascular disease in older adults. The Cardiovascular Health Study Research Group. Journal of the American Geriatrics Society, 48 (2), 115-23 PMID: 10682939
Baldwin CM, Ervin AM, Mays MZ, Robbins J, Shafazand S, Walsleben J, & Weaver T (2010). Sleep disturbances, quality of life, and ethnicity: the Sleep Heart Health Study. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine, 6 (2), 176-83 PMID: 20411696
Boulos MI, & Murray BJ (2010). Current evaluation and management of excessive daytime sleepiness. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques, 37 (2), 167-76 PMID: 20437926
Chokroverty S (2010). Overview of sleep & sleep disorders. The Indian journal of medical research, 131, 126-40 PMID: 20308738
Tuesday, May 18, 2010
How Chefs think about Size - Portion Size that is (another b2d nugget)
Follow @mcphoo
Tweet
"Despite the focus on the increase in portion sizes and the possible role in the development of obesity, little is known about how portion sizes are determined in restaurants." This is how an intriguing discussion of Chefs and their restaurant food size practices begins. The study aslo notes that eating out has gone up from 2.3x's a week in 1981 to 5 times in 2000. Within that period we know that standard dinner plates have gone from 10 to 12 inch plates. So what do chefs - the folks in the restaurant it turns out who set portion size - think of as "regular" sizes?
 Interestingly, chefs over 51 (trained in the smaller portion size era of the 70's) serve smaller sizes than younger chefs raised in the bigger portion period in which we find our super sized selves.
Interestingly, chefs over 51 (trained in the smaller portion size era of the 70's) serve smaller sizes than younger chefs raised in the bigger portion period in which we find our super sized selves.
If you think that Chefs are in the know about nutrition when it comes to food prep, this may be a leap of faith. The authors write:

What Motivates Chef Portion Size Selection? Survey says, not surprisingly: "presentation of food", cost, customer expectations. Competition and calorie count had only "some influence." But intriguingly, competition with other restaurants was strongly correlated with portion size of say pasta and steak. What's wild (ok, to me) is that where "customer expectiation" was high, larger veggie side plates were served BUT when calories were perceived to be a biggie, that's when veggie portion sizes got SMALLER. That's rather an interesting insight for what chefs might be taught, no?
And indeed, from the text above on portion sizes, restaurants are serving larger than 2-3oz of veggies - when they serve veggies - and what's wrong with that? 1/2 a cup is nothing. Bring it on - as long as it's sans the oil, butter, deep frying and etc's. Have the condiments on the side and add as necessary. Or not. But that is a topic for another day.
 Chef Perceptions: Here's something else interesting from the study: Chefs thought that patrons would notice if a serving size on their plate was 25% smaller - but a few things here: we are lousy at figuring size. And as we know from the last b2d post on energy density work, we can keep the plate looking just as full by using low energy dense foods, and folks can feel satisfied by same.
Chef Perceptions: Here's something else interesting from the study: Chefs thought that patrons would notice if a serving size on their plate was 25% smaller - but a few things here: we are lousy at figuring size. And as we know from the last b2d post on energy density work, we can keep the plate looking just as full by using low energy dense foods, and folks can feel satisfied by same.
What does this lack of knowledge in the kitchen mean for eating out? Be not afraid to ask the kitchen to put together something for you closer to your spec, and your sizes, perhaps. Putting together a variety of sides (smaller by nature than their full meal counter parts) can often be great. If you're anything like me - if it's in front of you, you'll eat it (interesting related work showing i fear i'm not unique in this) - so an easier thing for me is just not to have the bigger size in front of me and say "serve it, i just won't eat all of it"
Are these findings a surprise? That chefs (600 surveyed; 80% response rate) seem not to understand that veggies are largely low cal foods, or that their portion sizes are so out of whack with any recommendations for such sizes? Or is it to be expected that chefs simply learn what tastes good and how to prepare it in an appetising way, with younger chefs going for bigger sizes?
Does this mean it is all the more surprising that it was a chef, Jamie Oliver, who noticed the appalling quality of "school dinners" in the UK & now the US? That if a chef noticed, they must be truly terrible?
But perhaps more than anything else, this kind of survey means: trust no one. WHile the study's authors want to investigate ways to help chefs get up to speed with nutrition relative to the food they prepare, in the meantime, we need to educate ourselves about what's healthy or not; an appropriate portion or not, and perhaps what seems is a particular challenge for some folks, to make specific requests of a restaurant when eating out, based on that knowledge.
External Resources:
CITATIONS
If you think that Chefs are in the know about nutrition when it comes to food prep, this may be a leap of faith. The authors write:
An unexpected finding of this study was that chefs who reported that calorie content was an important factor when determining portion size reported serving a smaller portion of a vegetable side-dish, such as steamed broccoli, compared with chefs who did not identify calorie content as being important. This suggests that chefs do not understand that such vegetables are low in energy density and can help customers moderate energy intake.So, as we saw in the last b2d post about energy density rather than portion size being a big factor in successful weight management AND meal satisfaction, there's a huge whack of chefs who are failing on both energy density and portion size.

Figure Above: When chefs were asked to describe their perceptions of the average portion size of foods served in their establishments (Figure 1), the majority (76% ) reported serving "regular" portions, and <20% reported serving "large" or "extra-large" portions. When respondents were asked to estimate the typical portion size of penne pasta served in their restaurant, 4 oz (27% ), 6 oz (32% ), and 8 oz (18% ) portions were most frequently reported, with 90% of respondents serving portions larger than United States Department of Agriculture's recommendation of 1 oz. For strip steak, 48% of the respondents indicated that 12 oz steaks were typically served in their establishment, and 28% reporting 8 oz portions as being typical, with 83% of respondents serving portions that were larger than the 5.5 oz that the government recommends should be consumed each day. Most respondents (38% ) reported serving 3-oz portions of a vegetable side-dish, with 31% reporting 4-oz portions. Forty percent of these respondents served vegetable portions larger than United States Department of Agriculture's recommendation of ½ cup (2 to 3 oz). When asked about the size of plates used in their restaurants, 38% reported using 9.25- to 11-inch plates, and 33% reported using 11.25- to 13-inch plates.
What Motivates Chef Portion Size Selection? Survey says, not surprisingly: "presentation of food", cost, customer expectations. Competition and calorie count had only "some influence." But intriguingly, competition with other restaurants was strongly correlated with portion size of say pasta and steak. What's wild (ok, to me) is that where "customer expectiation" was high, larger veggie side plates were served BUT when calories were perceived to be a biggie, that's when veggie portion sizes got SMALLER. That's rather an interesting insight for what chefs might be taught, no?
And indeed, from the text above on portion sizes, restaurants are serving larger than 2-3oz of veggies - when they serve veggies - and what's wrong with that? 1/2 a cup is nothing. Bring it on - as long as it's sans the oil, butter, deep frying and etc's. Have the condiments on the side and add as necessary. Or not. But that is a topic for another day.
Chef Perceptions: Here's something else interesting from the study: Chefs thought that patrons would notice if a serving size on their plate was 25% smaller - but a few things here: we are lousy at figuring size. And as we know from the last b2d post on energy density work, we can keep the plate looking just as full by using low energy dense foods, and folks can feel satisfied by same.What does this lack of knowledge in the kitchen mean for eating out? Be not afraid to ask the kitchen to put together something for you closer to your spec, and your sizes, perhaps. Putting together a variety of sides (smaller by nature than their full meal counter parts) can often be great. If you're anything like me - if it's in front of you, you'll eat it (interesting related work showing i fear i'm not unique in this) - so an easier thing for me is just not to have the bigger size in front of me and say "serve it, i just won't eat all of it"
Are these findings a surprise? That chefs (600 surveyed; 80% response rate) seem not to understand that veggies are largely low cal foods, or that their portion sizes are so out of whack with any recommendations for such sizes? Or is it to be expected that chefs simply learn what tastes good and how to prepare it in an appetising way, with younger chefs going for bigger sizes?
Does this mean it is all the more surprising that it was a chef, Jamie Oliver, who noticed the appalling quality of "school dinners" in the UK & now the US? That if a chef noticed, they must be truly terrible?
TED prize winner, Jamie Oliver, giving his TED talk
But perhaps more than anything else, this kind of survey means: trust no one. WHile the study's authors want to investigate ways to help chefs get up to speed with nutrition relative to the food they prepare, in the meantime, we need to educate ourselves about what's healthy or not; an appropriate portion or not, and perhaps what seems is a particular challenge for some folks, to make specific requests of a restaurant when eating out, based on that knowledge.
External Resources:
- Precision Nutrition - free overview about painless healthy eating heuristics
- Georgie Fear's "Dig In" cook book - healthy AND tasty.
CITATIONS
Condrasky, M., Ledikwe, J., Flood, J., & Rolls, B. (2007). Chefs’ Opinions of Restaurant Portion Sizes* Obesity, 15 (8), 2086-2094 DOI: 10.1038/oby.2007.248
Harnack, L., Steffen, L., Arnett, D., Gao, S., & Luepker, R. (2004). Accuracy of estimation of large food portions☆ Journal of the American Dietetic Association, 104 (5), 804-806 DOI: 10.1016/j.jada.2004.02.026
Wansink B, Painter JE, & North J (2005). Bottomless bowls: why visual cues of portion size may influence intake. Obesity research, 13 (1), 93-100 PMID: 15761167Tweet Follow @begin2dig
Sunday, May 16, 2010
b2d nugget: portion size is out; energy density is in for effective weight management
Follow @mcphoo
Tweet
You'd think with bigger sizes, folks would feel more full after a feeding than with smaller sizes. Apparently not so.
In 2005, researchers were interested in whether the increase in portion size at restaurants and in snack foods was contributing to the obesity epidemic. Rightfully they acknowledge that while that would SEEM to make sense, it's tough to say so conclusively.
So what they did look at was - does eating more make one feel more full (and so maybe eat less at any point?). They also looked at "energy density" - how many calories are packed into a food item with the same weight (broccoli low ed; ice cream, high) - to see if that had an effect on fullness.

Here's the simple takeaway: big pig portions don't leave one more satisfied. But we all know small portions can leave one feeling well hungry. So, solution? Help folks start to mix in low energy dense foods, and that's way more successful than asking them to cut the fat. Guess what? weight loss ensues as their energy uptake (amount of calories a day) goes down.
Here's the abstract
 That last line says "eating satisfying portions" - which means that portions can still be pretty unfettered IF you're eating low energy density food. I wrote awhile ago how making mounds of greens super edible just by adding some really good balsamic vinegar. The beauty is, low energy density foods are also often HIGH in nutrient density. So, for instance, leafy greens are rich in macro and micronutrients while being low in kcals.
That last line says "eating satisfying portions" - which means that portions can still be pretty unfettered IF you're eating low energy density food. I wrote awhile ago how making mounds of greens super edible just by adding some really good balsamic vinegar. The beauty is, low energy density foods are also often HIGH in nutrient density. So, for instance, leafy greens are rich in macro and micronutrients while being low in kcals.
There's another related study in 2007 that shows however IF you can encourage folks to cut the fat a bit, after awhile, we don't miss it. So again another strategy towards saving kcals and weight management. Here's the abstract about how this finding was constucted:
That's cool. We happily adapt. SO of course someone had to look at the combination of some reduced fat and some engery density lowering foods together. Backlash? not at all. Good results:
The main thing in this last finding it seems is that again, we don't have to fiddle portion size on the plate particularly - which folks have a difficult time with as we looked at back when considering stupid set point theory - BUT get the mix of lowering fat and upping VOLUME of low energy dense food - which means good colours on the plate too, that we get to reduced caloric intake without feeling like we're starving.
Related resources:
Citations
In 2005, researchers were interested in whether the increase in portion size at restaurants and in snack foods was contributing to the obesity epidemic. Rightfully they acknowledge that while that would SEEM to make sense, it's tough to say so conclusively.
So what they did look at was - does eating more make one feel more full (and so maybe eat less at any point?). They also looked at "energy density" - how many calories are packed into a food item with the same weight (broccoli low ed; ice cream, high) - to see if that had an effect on fullness.
british nutrition foundation "feed yourself fuller" chart
Here's the simple takeaway: big pig portions don't leave one more satisfied. But we all know small portions can leave one feeling well hungry. So, solution? Help folks start to mix in low energy dense foods, and that's way more successful than asking them to cut the fat. Guess what? weight loss ensues as their energy uptake (amount of calories a day) goes down.
Here's the abstract
The increase in the prevalence of obesity has coincided with an increase in portion sizes of foods both inside and outside the home, suggesting that larger portions may play a role in the obesity epidemic. Although it will be difficult to establish a causal relationship between increasing portion size and obesity, data indicate that portion size does influence energy intake. Several well-controlled, laboratory-based studies have shown that providing older children and adults with larger food portions can lead to significant increases in energy intake. This effect has been demonstrated for snacks and a variety of single meals and shown to persist over a 2-d period. Despite increases in intake, individuals presented with large portions generally do not report or respond to increased levels of fullness, suggesting that hunger and satiety signals are ignored or overridden. One strategy to address the effect of portion size is decreasing the energy density (kilojoules per gram; kilocalories per gram) of foods. Several studies have demonstrated that eating low-energy-dense foods (such as fruits, vegetables, and soups) maintains satiety while reducing energy intake. In a clinical trial, advising individuals to eat portions of low-energy-dense foods was a more successful weight loss strategy than fat reduction coupled with restriction of portion sizes. Eating satisfying portions of low-energy-dense foods can help to enhance satiety and control hunger while restricting energy intake for weight management.
There's another related study in 2007 that shows however IF you can encourage folks to cut the fat a bit, after awhile, we don't miss it. So again another strategy towards saving kcals and weight management. Here's the abstract about how this finding was constucted:
This study establishes the reliability and validity of the Fat Preference Questionnaire©, a self-administered instrument to assess preference for dietary fat. Respondents select the food which tastes better and is eaten more frequently from 19 sets of food. Each set is comprised of related foods differing in fat content. The questionnaire was administered to women in laboratory-based (n=63), cross-sectional (n=150), and weight-loss (n=71) studies. The percentage of food sets in which high-fat foods were reported to “taste better” (TASTE score) and to be “eaten more often” (FREQ score) was determined. A measure of dietary fat restriction (DIFF) was created by subtracting TASTE from FREQ. Food intake was assessed by direct measure, 24-h recall, or food diary. Additionally, participants completed a standard survey assessing dietary restraint. Test–retest correlations were high (r=0.75–0.94). TASTE and FREQ scores were positively correlated with total fat intake (r=0.22–0.63). DIFF scores positively correlated with dietary restraint (r=0.39–0.52). Participants in the weight-loss trial experienced declines in fat consumption, TASTE and FREQ scores, and BMI values, and an increase in DIFF scores. Weight loss correlated with declines in FREQ (r=0.36) scores and increases in DIFF scores (r=−0.35). These data suggest that preference for dietary fat declines when following a reduced-fat diet and an increase in restraint for intake of dietary fat is important for weight loss. The Fat Preference Questionnaire© is a stable, easily-administered instrument that can be used in research and clinical settings.
That's cool. We happily adapt. SO of course someone had to look at the combination of some reduced fat and some engery density lowering foods together. Backlash? not at all. Good results:
BACKGROUND: Consuming foods low in energy density (kcal/g) decreases energy intake over several days, but the effectiveness of this strategy for weight loss has not been tested. OBJECTIVE: The effects on weight loss of 2 strategies for reducing the energy density of the diet were compared over 1 y. DESIGN: Obese women (n = 97) were randomly assigned to groups counseled either to reduce their fat intake (RF group) or to reduce their fat intake and increase their intake of water-rich foods, particularly fruit and vegetables (RF+FV group). No goals for energy or fat intake were assigned; the subjects were instructed to eat ad libitum amounts of food while following the principles of their diet. RESULTS: After 1 y, study completers (n = 71) in both groups had significant decreases in body weight (P < 0.0001). Subjects in the RF+FV group, however, had a significantly different pattern of weight loss (P = 0.002) than did subjects in the RF group. After 1 y, the RF+FV group lost 7.9 +/- 0.9 kg and the RF group lost 6.4 +/- 0.9 kg. Analysis of all randomly assigned subjects also showed a different pattern of weight loss between groups (P = 0.021). Diet records indicated that both groups had similar reductions in fat intake. The RF+FV group, however, had a lower dietary energy density than did the RF group (P = 0.019) as the result of consuming a greater weight of food (P = 0.025), especially fruit and vegetables (P = 0.037). The RF+FV group also reported less hunger (P = 0.003). CONCLUSION: Reducing dietary energy density, particularly by combining increased fruit and vegetable intakes with decreased fat intake, is an effective strategy for managing body weight while controlling hunger.
The main thing in this last finding it seems is that again, we don't have to fiddle portion size on the plate particularly - which folks have a difficult time with as we looked at back when considering stupid set point theory - BUT get the mix of lowering fat and upping VOLUME of low energy dense food - which means good colours on the plate too, that we get to reduced caloric intake without feeling like we're starving.
Related resources:
- b2d nutrition index
- respect the fat
- what's a "whole protein" - esp. going veggie
- set point theory is crap
- why is fish oil anti-inflamatory?
Citations
Ello-Martin JA, Ledikwe JH, & Rolls BJ (2005). The influence of food portion size and energy density on energy intake: implications for weight management. The American journal of clinical nutrition, 82 (1 Suppl) PMID: 16002828Tweet Follow @begin2dig
LEDIKWE, J., ELLOMARTIN, J., PELKMAN, C., BIRCH, L., MANNINO, M., & ROLLS, B. (2007). A reliable, valid questionnaire indicates that preference for dietary fat declines when following a reduced-fat diet Appetite, 49 (1), 74-83 DOI: 10.1016/j.appet.2006.12.001
Ello-Martin JA, Roe LS, Ledikwe JH, Beach AM, & Rolls BJ (2007). Dietary energy density in the treatment of obesity: a year-long trial comparing 2 weight-loss diets. The American journal of clinical nutrition, 85 (6), 1465-77 PMID: 17556681
Subscribe to:
Posts (Atom)
 COACHING with dr. m.c.
COACHING with dr. m.c. 


