Showing posts with label injury. Show all posts
Showing posts with label injury. Show all posts
Saturday, July 31, 2010
Tempo as bulletproofing - at how many speeds do we practice a move?
Follow @mcphoo
Tweet
When we think about speed - we usually think about one direction: going fast. Acceleration. Explosion. But it seems there is benefit to rethinking a little bit the roll of speed in our practice in terms of what we want to achieve beyond or even within the faster finish, the bigger lift, the quicker 40. Control at ranges of speed - including the super fast of the sport speed is skill work that may also not only make us better athletes but protect us from movement-based injury.
The Big Lift. If we lift stuff, we generally practice lifting at the speed we think best for our goals: in lifting we hear a lot about acceleration. Get up as fast as possible; put the thing up as fast as possible. Explode explode. And with good physics behind that: acceleration is part of Force, so the more we can get speed to ramp up, the more force the more we lift.

The debates about speed optimisation for hypertrophy are legion: x seconds up y seconds down. What's best? Well, what are we trying to do? Me, for hypertrophy, i do like Chad Waterbury's Huge in a Hurry
for hypertrophy, i do like Chad Waterbury's Huge in a Hurry with its use of a punchy tempo, sticking with that, and dropping weight if the tempo goes down (book overview by Waterbury). Waterbury's goal, he says, is to recruit as much muscle fiber as possible.
with its use of a punchy tempo, sticking with that, and dropping weight if the tempo goes down (book overview by Waterbury). Waterbury's goal, he says, is to recruit as much muscle fiber as possible.
While Waterbury's article doesn't explain how that happens, here's an idea to do with energy systems and fiber types: faster muscle fibers (type II's mainly) that are used first in a fast burst of force can give lots of energy to power work. They're also the ones that hypertrophy particularly well.
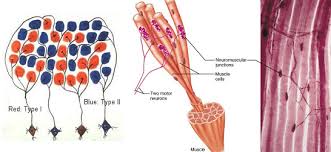 Those fibers, however, fatigue out fastest though. 10secs of work for Type IIa's; Type IId's go for about 30secs. As they fatigue other muscle fibers (Type I, slower but longer lasting ) come on. Hence more sets: initial sets do the fatiguing with dominant one type of fiber; later sets get more muscle fibers, too but of a different type. Even with recovery of 30 secs between longer rep sets, we are only partially recovering that IId energy system - and that's a good thing: better fiber mix, better strength/hypertrophy response.
Those fibers, however, fatigue out fastest though. 10secs of work for Type IIa's; Type IId's go for about 30secs. As they fatigue other muscle fibers (Type I, slower but longer lasting ) come on. Hence more sets: initial sets do the fatiguing with dominant one type of fiber; later sets get more muscle fibers, too but of a different type. Even with recovery of 30 secs between longer rep sets, we are only partially recovering that IId energy system - and that's a good thing: better fiber mix, better strength/hypertrophy response.
In other sports, too, it's speed that wins the race. Even in endurance sports, it's still who crosses the line first that counts. Very linear, these things.
So fast sounds great. Why go slow(er)? Control!
While there's a nice linear cross the finish line first in many sports, other games require other tempos to be available at all times, don't they? Scoring in baseball, football, rugby definitely has speed as a component, but it's not always the fastest person who sets up the goal, or scores the run, is it? Great tennis players are able to move very fast, but they are also able to control ball position to the opponents court at slower speeds, giving their oponent less energy on that ball either to get to it or return it. That takes control.

To attain that control, it seems we're actually using different muscle patterns. Not only that, muscle patterns change with practice. IF we only practice at one tempo we will not be as comfortable or smooth or controlled at those different speeds, and so if that different tempo is required of us, we may not be as effective as we would like to be, especially through a full range of motion.
By not training at different speeds, we therefore miss out on opportunities to get stronger, use a richer variety of fibers and, perhaps especially, have that advanced control of our bodies - something that comes in extremely handy when the ground shifts from under us either on a bouncy bus, or rolling over a divot in the grass, or making that weird pass around an oncoming player in an Ultimate game.
Finding the Weak Spots and Improving their Performance. While different speeds helps us learn how to control our bodies at different paces, and thus gives us a greater skills palette, we can also find holes in our range of motion control by practicing at a variety of speeds, where, what direction and at what tempo do we hit a movement dead zone for instance, where control seems to fall off? Let's bring some focused attention and practice to that part of the movement at that tempo.
Sloooow Speed for Skill Building. An oft-cited example by folks who love training at speed variety is Ben Hogan and his slow motion swing work. One of the best golfers of the game, with perhaps the most admired swing, he reputedly practiced regularly going through each part of his swing with intent, as shown below, with the miracle of youtube:
Even No Speed
Relatively recent research has also shown that mental imagery practice, while not effecting reaction speed, does effect muscle strength, power and work "signficantly."
Technique Challenge: use a metronome
During the S-Phase Z-Health course (yup, S is pretty much for Skills for Speed), we did some great speed work that was about using a metronome to get used to working at differnt tempi than those to which we are accustomed (i.e. in a rut). Our practice was to do mobility drills to the tempo of the metronome.
Not too suprisingly, folks who dance or play an instrument seemed more at ease with the exercise, but even here, working outside familiar pacing (103 beats per minute, anyone?) was more of a challenge than standard quarters and thirds.
Practicing Speed at all Joints and Loads of Angles
Z-Health's R-Phase (overview) and I-Phase programs (overview) are dynamic joint movement programs. The DVD's for each take us through each joint in the body and we do a sequence of movments for each to get the various ranges of motion. R-Phase does all the movements from neutral stance; I-phase gets going with a variety of stances and positions. Getting from R to I is a good idea for having the mastery to apply the movements to sport specific actions.
 While the DVDs show a single speed for each drill, the manuals describing the training programs for each make it clear that the drills are designed to be "owned" at at least 4 speeds from super slow to "sports speed" (really fast). Control control control. The brain maps not only position of where we are but how fast we're moving each part of us to get there. Practicing speeds builds patterns for managing actions at speeds.
While the DVDs show a single speed for each drill, the manuals describing the training programs for each make it clear that the drills are designed to be "owned" at at least 4 speeds from super slow to "sports speed" (really fast). Control control control. The brain maps not only position of where we are but how fast we're moving each part of us to get there. Practicing speeds builds patterns for managing actions at speeds.
Once these drills/speeds are owned, S-Phase: the Complete Athlete Vol 1 puts these drills into more loaded conditions for actual full body speed/tempo work.
 Side Note: If you're intrigued by these progressions in control/speed for each joint ROM, the speediest way to get a primer in them is either the Essentials of Elite Performance 3day workshop (calendar here) or DVD mini course, distilled from the workshop (overview), if you can't make the event.
Side Note: If you're intrigued by these progressions in control/speed for each joint ROM, the speediest way to get a primer in them is either the Essentials of Elite Performance 3day workshop (calendar here) or DVD mini course, distilled from the workshop (overview), if you can't make the event.
Summary
There are it seems specific speed combinations that lead to specific effects. Being able to use speed in a controlled way to achieve those effects is a Good Thing. But part of having control of speed at one end of the spectrum (the fast end) seems to be pretty tied up with the neural patterning that goes on to control speed at t'other end (very slow) too.
Adding in speed work - where speed means from the slow to the fast - as part of our regular practice may just be one more way to improve our overall well-being and bullet proof ourselves better against the unexpected - when that unexpected requires a movement response. Tweet Follow @begin2dig
The Big Lift. If we lift stuff, we generally practice lifting at the speed we think best for our goals: in lifting we hear a lot about acceleration. Get up as fast as possible; put the thing up as fast as possible. Explode explode. And with good physics behind that: acceleration is part of Force, so the more we can get speed to ramp up, the more force the more we lift.
The debates about speed optimisation for hypertrophy are legion: x seconds up y seconds down. What's best? Well, what are we trying to do? Me,
While Waterbury's article doesn't explain how that happens, here's an idea to do with energy systems and fiber types: faster muscle fibers (type II's mainly) that are used first in a fast burst of force can give lots of energy to power work. They're also the ones that hypertrophy particularly well.
In other sports, too, it's speed that wins the race. Even in endurance sports, it's still who crosses the line first that counts. Very linear, these things.
So fast sounds great. Why go slow(er)? Control!
While there's a nice linear cross the finish line first in many sports, other games require other tempos to be available at all times, don't they? Scoring in baseball, football, rugby definitely has speed as a component, but it's not always the fastest person who sets up the goal, or scores the run, is it? Great tennis players are able to move very fast, but they are also able to control ball position to the opponents court at slower speeds, giving their oponent less energy on that ball either to get to it or return it. That takes control.
To attain that control, it seems we're actually using different muscle patterns. Not only that, muscle patterns change with practice. IF we only practice at one tempo we will not be as comfortable or smooth or controlled at those different speeds, and so if that different tempo is required of us, we may not be as effective as we would like to be, especially through a full range of motion.
By not training at different speeds, we therefore miss out on opportunities to get stronger, use a richer variety of fibers and, perhaps especially, have that advanced control of our bodies - something that comes in extremely handy when the ground shifts from under us either on a bouncy bus, or rolling over a divot in the grass, or making that weird pass around an oncoming player in an Ultimate game.
Finding the Weak Spots and Improving their Performance. While different speeds helps us learn how to control our bodies at different paces, and thus gives us a greater skills palette, we can also find holes in our range of motion control by practicing at a variety of speeds, where, what direction and at what tempo do we hit a movement dead zone for instance, where control seems to fall off? Let's bring some focused attention and practice to that part of the movement at that tempo.
Sloooow Speed for Skill Building. An oft-cited example by folks who love training at speed variety is Ben Hogan and his slow motion swing work. One of the best golfers of the game, with perhaps the most admired swing, he reputedly practiced regularly going through each part of his swing with intent, as shown below, with the miracle of youtube:
Even No Speed
Relatively recent research has also shown that mental imagery practice, while not effecting reaction speed, does effect muscle strength, power and work "signficantly."
Technique Challenge: use a metronome
During the S-Phase Z-Health course (yup, S is pretty much for Skills for Speed), we did some great speed work that was about using a metronome to get used to working at differnt tempi than those to which we are accustomed (i.e. in a rut). Our practice was to do mobility drills to the tempo of the metronome.
Not too suprisingly, folks who dance or play an instrument seemed more at ease with the exercise, but even here, working outside familiar pacing (103 beats per minute, anyone?) was more of a challenge than standard quarters and thirds.
Practicing Speed at all Joints and Loads of Angles
Z-Health's R-Phase (overview) and I-Phase programs (overview) are dynamic joint movement programs. The DVD's for each take us through each joint in the body and we do a sequence of movments for each to get the various ranges of motion. R-Phase does all the movements from neutral stance; I-phase gets going with a variety of stances and positions. Getting from R to I is a good idea for having the mastery to apply the movements to sport specific actions.
Once these drills/speeds are owned, S-Phase: the Complete Athlete Vol 1 puts these drills into more loaded conditions for actual full body speed/tempo work.
Summary
There are it seems specific speed combinations that lead to specific effects. Being able to use speed in a controlled way to achieve those effects is a Good Thing. But part of having control of speed at one end of the spectrum (the fast end) seems to be pretty tied up with the neural patterning that goes on to control speed at t'other end (very slow) too.
Adding in speed work - where speed means from the slow to the fast - as part of our regular practice may just be one more way to improve our overall well-being and bullet proof ourselves better against the unexpected - when that unexpected requires a movement response. Tweet Follow @begin2dig
Wednesday, April 21, 2010
Ankle Sprains: Tape, Bracing - doesn't matter finds research - but how'd we get so busted up in the first place?
Follow @mcphoo
Tweet

 A recent paper has presented the results of a bunch of trials looking at interventions for ankle sprains. Main result? if someone's had an ankle injury - like a sprain - then tape or brace doesn't seem to show a difference: both seem to cut down reinjury. What's troublesome on a metalevel, is first how sort of accepted the notion of this level of injury seems to be, and second how nascent in the approach described here is the model that for folks who haven't been injured - as a preventitive - they maybe should be immobilised too. Aren't there other questions to ask - perhaps especially about the injury free staying injury free - rather than whether incapacitating natural function is a Good Idea? But perhaps more fundamentally, how did we get to this point where someone is so beaten up their joints are written off as so dysfunctional they must be immobilized to perform?
A recent paper has presented the results of a bunch of trials looking at interventions for ankle sprains. Main result? if someone's had an ankle injury - like a sprain - then tape or brace doesn't seem to show a difference: both seem to cut down reinjury. What's troublesome on a metalevel, is first how sort of accepted the notion of this level of injury seems to be, and second how nascent in the approach described here is the model that for folks who haven't been injured - as a preventitive - they maybe should be immobilised too. Aren't there other questions to ask - perhaps especially about the injury free staying injury free - rather than whether incapacitating natural function is a Good Idea? But perhaps more fundamentally, how did we get to this point where someone is so beaten up their joints are written off as so dysfunctional they must be immobilized to perform?
Here's the abstract:
So what's going on here that this is even considered a useful strategy?
Apparently, there's a lot of functional instability, mechanical and proprioceptive factors are also considered in some of the studies to be impaired. Mechanical instability (lax joint) can be a cause of functional instability. These effects build up from - you guessed it - repeated ankle injuries. Where reflexes get slower, joints can get hypermobile, funtional loss of static and dynamic support of the joint has gone way down. Effectively, the ankle for a potential variety of reasons, is so beaten up and abused, it can no long function as an ankle, so, a greater degree of immobility is preferable to too much.
Um. what happened that a person gets to this point of so MANY repeated injuries they're beyond the pale of recovering normal function? Ah right: this is sport, not health.
Intriguingly, there's a claim that some bracing helps proprioception:
There are alternatives approaches: perhaps we should ask, as indicated, what's causing these injuries in the first place? Is it a skills-on-the-field problem? turning skills? cognitive processing for field awareness skills? Is it lack of ankle flexion or hip/pelvis restrictions? Is it a sensory-motor disconnect with shoes or other gear killing proprioceptive awareness of foot placement?
Folks like Gray Cook working with NFL football teams have been looking at athletic mobility/stability. Eric Cobb has been looking more at sensory-motor approaches, and cognitive stress for field performance that's more effective and injury free.
Any solution assumes a model for which that solution is appropriate. The solutions proposed by these authors seems to presuppose a model where (a) the amount of reinjury that leads to such horrible dysfunction is taken as a given and seems to be ok such that (b) further bodily immobilization seems like a good idea to enable athletic movement seems problematic to me on a number of levels.
Strategies to understand why the injuries are so high in the first place - never mind acceptable - seems to be a more humane way to begin strategizing about enabling athltetes to play ball, no?
Related Posts
Citation
Dizon, J., & Reyes, J. (2010). A systematic review on the effectiveness of external ankle supports in the prevention of inversion ankle sprains among elite and recreational players Journal of Science and Medicine in Sport, 13 (3), 309-317 DOI: 10.1016/j.jsams.2009.05.002 Tweet Follow @begin2dig
Here's the abstract:
Epidemiological studies have shown that 10–28% of all sports injuries are ankle sprains, leading to the longest absence from athletic activity compared to other types of injuries. This study was conducted to evaluate the effectiveness of external ankle supports in the prevention of inversion ankle sprains and identify which type of ankle support was superior to the other. A search strategy was developed, using the keywords, ankle supports, ankle brace, ankle tapes, ankle sprains and athletes, to identify available literature in the databases (MEDLINE, PubMed, CINAHL, EMBASE, etc.), libraries and unpublished papers. Trials which consider adolescents and adults, elite and recreational players as participants were the study of choice. External ankle supports comprise ankle tape, brace or orthosis applied to the ankle to prevent ankle sprains. The main outcome measures were frequency of ankle sprains. Two reviewers assessed the quality of the studies included using the Joanna Briggs Institute (JBI Appraisal tool). Whenever possible, results were statistically pooled and interpreted. A total of seven trials were finally included in this study. The studies included were of moderate quality, with blinding as the hardest criteria to fulfill. The main significant finding was the reduction of ankle sprain by 69% (OR 0.31, 95% CI 0.18–0.51) with the use of ankle brace and reduction of ankle sprain by 71% (OR 0.29, 95% CI 0.14–0.57) with the use of ankle tape among previously injured athletes. No type of ankle support was found to be superior than the other.This is when it's nice to have the whole article, because you'd think it just stops there, right? For previously injured, folks who were taped didn't seem to get reinjured. How does one predict the future like that? Well that's the toughie: only one study had a control group - so did they just get reinjured that many more times than the athletes who braced? No, it's of the populations taped or braced, how many did NOT have a recurrence in a given period.
So what's going on here that this is even considered a useful strategy?
Apparently, there's a lot of functional instability, mechanical and proprioceptive factors are also considered in some of the studies to be impaired. Mechanical instability (lax joint) can be a cause of functional instability. These effects build up from - you guessed it - repeated ankle injuries. Where reflexes get slower, joints can get hypermobile, funtional loss of static and dynamic support of the joint has gone way down. Effectively, the ankle for a potential variety of reasons, is so beaten up and abused, it can no long function as an ankle, so, a greater degree of immobility is preferable to too much.
Um. what happened that a person gets to this point of so MANY repeated injuries they're beyond the pale of recovering normal function? Ah right: this is sport, not health.
Intriguingly, there's a claim that some bracing helps proprioception:
"they restrict range of motion to a certain degree and enhance proprioception of the injured ankle making them more useful in the prevention of possible re-injury."Wow, that's wild. How does that work? And can that awareness be re-trained rather than delivered only through a device? Where's it coming from? But there's not a lot of interest in the article in looking at say other strategies like rehab, movement assessment. Why not? There's a model here that says once injured, you're toasted:
As mentioned earlier in the discussion, after a sprain, structural damage occurs to the ligamentous tissues, nervous and musculo- tendinous units in the ankle joint. Functional and mechanical instability arise. For these reasons, the risk of injury to a pre- viously injured ankle is increased. his is the point where external ankle supports play an important role.And that may have informed the authors' decision simply to look at what type of bracing is better to reduce re-injury, rather than to wonder if
- training that can find movement or other sensory-motor issues that may be related to WHY a person roles their ankles
- investigation of the stupid shoes that may be killing proprioception necessary to reduce ankle sprains
- anything else that may help the athlete perform with less likelihood of injury, better performance
This review provides good evidence for the use either ankle taping or ankle braces to prevent lateral ankle sprains among previously injured players. However, for those with- out previous ankle injuries this still needs to be proven. There is no evidence on which external ankle support is better than the other. Each has its own advantages and disadvantages.You see it? These folks with this model of the weakness of the ankle - where "10-28%" of all athletic injuries occur - are already thinking MAYBE - we don't know yet - but maybe if we just brace the ankle up from the get go, we'll keep more ankles from being sprained.
There are alternatives approaches: perhaps we should ask, as indicated, what's causing these injuries in the first place? Is it a skills-on-the-field problem? turning skills? cognitive processing for field awareness skills? Is it lack of ankle flexion or hip/pelvis restrictions? Is it a sensory-motor disconnect with shoes or other gear killing proprioceptive awareness of foot placement?
Folks like Gray Cook working with NFL football teams have been looking at athletic mobility/stability. Eric Cobb has been looking more at sensory-motor approaches, and cognitive stress for field performance that's more effective and injury free.
Any solution assumes a model for which that solution is appropriate. The solutions proposed by these authors seems to presuppose a model where (a) the amount of reinjury that leads to such horrible dysfunction is taken as a given and seems to be ok such that (b) further bodily immobilization seems like a good idea to enable athletic movement seems problematic to me on a number of levels.
Strategies to understand why the injuries are so high in the first place - never mind acceptable - seems to be a more humane way to begin strategizing about enabling athltetes to play ball, no?
Related Posts
Citation
Dizon, J., & Reyes, J. (2010). A systematic review on the effectiveness of external ankle supports in the prevention of inversion ankle sprains among elite and recreational players Journal of Science and Medicine in Sport, 13 (3), 309-317 DOI: 10.1016/j.jsams.2009.05.002 Tweet Follow @begin2dig
Tuesday, July 28, 2009
If you're in an arm cast consider creatine to keep up your muscle
Follow @mcphoo
Tweet
Here's a very simple find that seems intriguing. Say your arm is in a cast and you can't work  out. The old saw in muscle work is use it or lose it.
out. The old saw in muscle work is use it or lose it.
Turns out, at least for young men who haven't done creatine before, that doing *some* creatine supplementation makes a difference in terms of preserving lean tissue in the upper limbs.
The authors caution that results by others of testing lower limb immobilization has not found these results. They wonder if it's the ratio of fiber types in the upper limbs or other factors that show these results. Suffice it to say, if you find yourself in an arm cast, you may want to consider trying some creatine to reduce "myoplastic changes directly related to disuse atrophy, thereby facilitating the rehabilitation process."
Just be sure to get a good quality creatine :) Tweet Follow @begin2dig
out. The old saw in muscle work is use it or lose it.Turns out, at least for young men who haven't done creatine before, that doing *some* creatine supplementation makes a difference in terms of preserving lean tissue in the upper limbs.
Johnston, APW, Burke, DG, MacNeil, LG, and Candow, DG. Effect of creatine supplementation during cast-induced immobilization on the preservation of muscle mass, strength, and endurance. J Strength Cond Res 23(1): 116-120, 2009-
Muscle and strength loss will occur during periods of physical inactivity and immobilization. Creatine supplementation may have a favorable effect on muscle mass and strength independently of exercise. The purpose of this study was to determine the effects of creatine supplementation on upper-limb muscle mass and muscle performance after immobilization. Before the study, creatine-naive men (n = 7; 18-25 years) were assessed for lean tissue mass (dual-energy X-ray absorptiometry), strength (1-repetition maximum [1RM] isometric single arm elbow flexion/extension), and muscle endurance (maximum number of single-arm isokinetic elbow flexion/extension repetitions at 60% 1RM). After baseline measures, subjects had their dominant or nondominant (random assignment) upper limb immobilized (long arm plaster cast) at 90[degrees] elbow flexion. Using a single-blind crossover design, subjects received placebo (maltodextrin; 4 x 5 g[middle dot]d-1) during days 1-7 and creatine (4 x 5 g[middle dot]d-1) during days 15-21. The cast was removed during days 8-14 and 22-29. The dependent measures of lean tissue mass, strength, and endurance were assessed at baseline, postcast, and after the study. During immobilization, compared with isocaloric placebo, creatine supplementation better maintained lean tissue mass (Cr +0.9% vs. PLA -3.7%, p
The authors caution that results by others of testing lower limb immobilization has not found these results. They wonder if it's the ratio of fiber types in the upper limbs or other factors that show these results. Suffice it to say, if you find yourself in an arm cast, you may want to consider trying some creatine to reduce "myoplastic changes directly related to disuse atrophy, thereby facilitating the rehabilitation process."
Just be sure to get a good quality creatine :) Tweet Follow @begin2dig
Subscribe to:
Posts (Atom)
 COACHING with dr. m.c.
COACHING with dr. m.c. 


